Article Text

Statistics from Altmetric.com
- abortion
- induced
- family planning services
- health services accessibility
- obesity
- maternal
- reproductive health services
- reproductive health
Private, independent clinics provide 59% of US abortions annually, and 60% are surgical procedures.1 Access to timely abortion is important, especially for people with medical conditions at increased risk for pregnancy-related physiological changes that exacerbate chronic conditions and morbidity and mortality associated with pregnancy.2 There are preexisting conditions that render community-based surgical abortion unsafe; however, referral to hospital-based care results in delay, increased risk, stigma, and cost at later gestations.3 Patients with stigmatised medical conditions like obesity and substance use disorder may be over-referred for hospital-based care due to provider bias, rather than increased risk of procedural complication.2
In our independent abortion clinic, eligibility screening for community-based procedures is conducted by telephone at time of appointment request for abortion up to 23 weeks 6 days’ gestation. We excluded medical abortion in this report. The Medical Director rules patients as eligible or ineligible for abortion. Staff place referrals to a hospital near the clinic for patients deemed ineligible for community-based abortion.
To improve our screening and referral process we conducted a retrospective audit by reviewing the screening forms for patients referred out of our clinic from 2012 to 2018. To understand our ineligibility criteria patterns we categorised the reasons for referral as: (1) obesity, (2) substance use, (3) bleeding risk (eg, reported anaemia or bleeding dycrasias), (4) gestational age, (5) other (eg, heart disease, venous thromboembolism/stroke, epilepsy, moderate or severe asthma, diabetes, liver disease, hypertension) or (6) unclear reason. We performed descriptive statistics to characterise the reasons for referral and employed the Cochran–Armitage trend test to assess referral indications over time.
A total of 14 516 patients sought surgical abortion over the study period. We placed referrals to hospital-based, third-trimester abortion or prenatal care for 516 (3.5%) patients.
The abortion rate declined in our state in this period, in parallel with a nationwide drop in abortions simultaneous with a rise in use of highly effective contraception.4 Despite this trend, there was a statistically significant decline over the study period in the total number of patients referred elsewhere (p<0.0001) (figure 1). Analysis of our complications over the same study period was reported previously5 and our relaxed eligibility criteria did not negatively affect our complication rate.
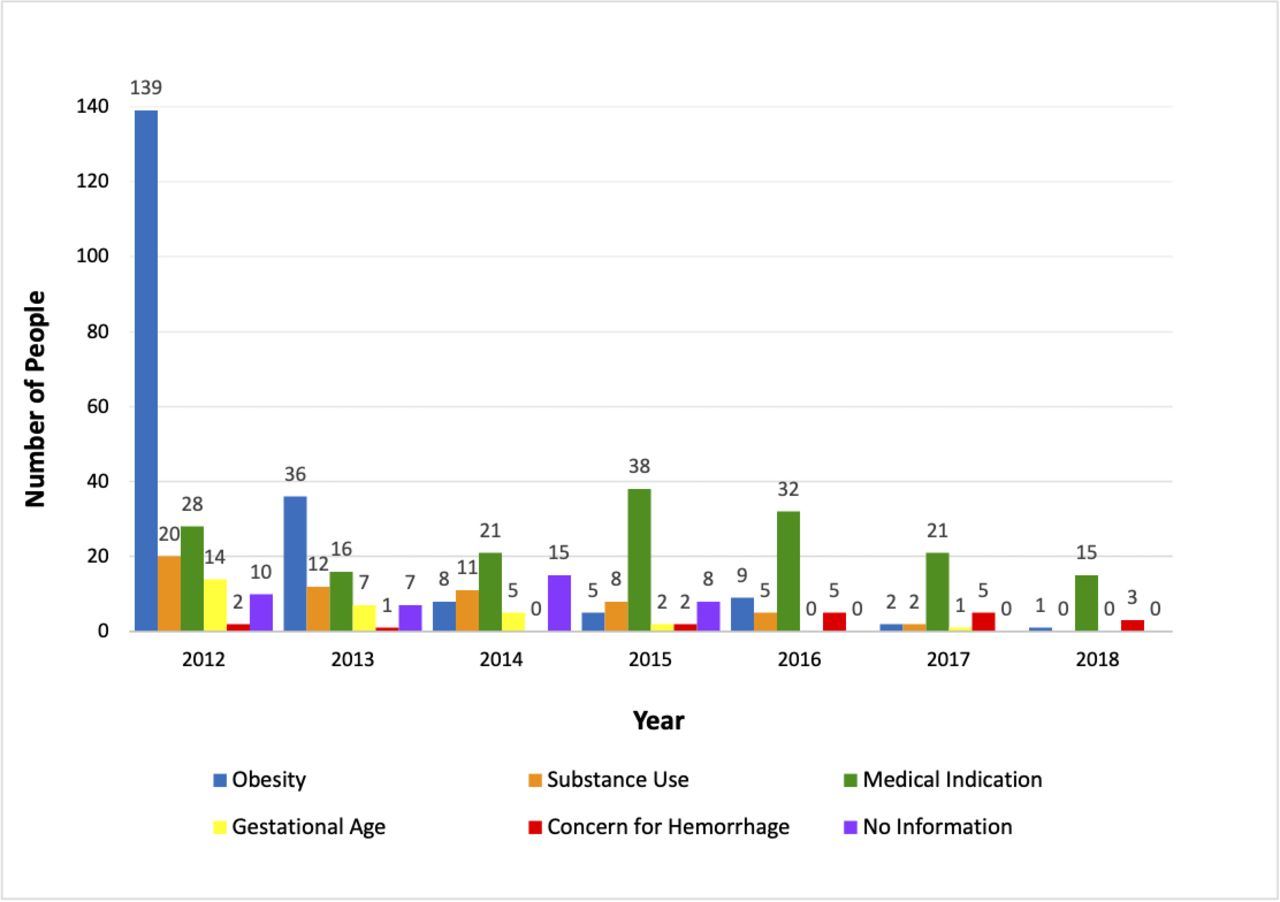
{kind=link}
Number of patients referred elsewhere for specific ineligibility criteria by year (n=516).
Prior to 2012, all patients with a body mass index (BMI) over 35 kg/m2 and patients with substance use disorder not on maintenance therapy were referred for hospital-based care. As obesity and substance use disorder became more common in our community, we redrafted our eligibility guidelines to be more patient-centred for a greater proportion of our population. We deliberately changed our protocols so that obesity alone at any BMI was not disqualifying for care. Furthermore, we provided abortion to patients who reported substance use with a negative urine toxicology on the day of their appointment. Increased comfort among gynaecology and anaesthesia staff with patients with complex medical conditions resulted in fewer referrals to hospital-based care.
It is critical that community-based abortion remains accessible for medically complex patients, as referral to hospital-based care raises cost and incurs delay, which increases procedure risk. We encourage other community-based abortion providers to understand population frequencies of common medical conditions within their catchment area and reconsider protocols that may be unnecessarily strict. We would like to emphasise the importance of review of criteria for referral to hospital-based care, especially for stigmatised diseases like obesity and substance use disorder, which have the potential to be over-referred for hospital-based care due to provider bias.2
Ethics statements
Patient consent for publication
Footnotes
Twitter @AliceMAbernathy
Contributors AA collected and reviewed data and authored the manuscript; MS collected data and secured funding for the project; RM conducted statistical analysis of the data; EJ supervised data analysis and edited the work; LD-B provided clinical data; DB was the primary investigator and editor and secured funding for the project.
Funding This research was supported by a departmental grant from Brigham and Women’s Hospital Department of Obstetrics and Gynecology.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; internally peer reviewed.