Article Text

Abstract
Background This systematic review aimed to identify and describe the factors that influence female genital mutilation/cutting (FGM/C).
Methods Searches were conducted in Medline, PsycInfo, Web of Science, Embase and the grey literature from 2009 to March 2020 with no language restrictions, using related MESH terms and keywords. Studies were included if they were quantitative and examined factors associated with FGM/C. Two researchers independently screened studies for inclusion, extracted data and assessed study quality. The direction, strength and consistency of the association were evaluated for determinants, presented as a descriptive summary, and were disaggregated by age and region.
Results Of 2230 studies identified, 54 published articles were included. The majority of studies were from the African Region (n=29) followed by the Eastern Mediterranean Region (n=18). A lower level of maternal education, family history of FGM/C, or belonging to the Muslim religion (in certain contexts) increased the likelihood of FGM/C. The majority of studies that examined higher paternal education (for girls only) and living in an urban region showed a reduced likelihood of FGM/C, while conflicting evidence remained for wealth. Several studies reported that FGM/C literacy, and low community FGM/C prevalence were associated with a reduced likelihood of FGM/C.
Conclusions There were several characteristics that appear to be associated with FGM/C, and these will better enable the targeting of policies and interventions. Importantly, parental education may be instrumental in enabling communities and countries to meet the Sustainable Development Goals.
- epidemiology
- circumcision, female
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
This systematic review identified 54 articles; most studies were from the African Region, were household surveys and used self-report of female genital mutilation (FGM).
Higher levels of parental education appeared to be protective against FGM in the majority of studies that examined this factor.
Most studies identified that family history of FGM, living in a rural area, and having specific religious beliefs increased the likelihood of FGM.
Introduction
Female genital mutilation (FGM), also known as female genital cutting (FGC), refers to procedures that involve alteration of female genitalia without a medical or therapeutic reason.1 The United Nations Sustainable Development Goals (SDG target: 5.3) calls for ending FGM/C as a harmful traditional practice against women and girls by 2030.2 The World Health Organization (WHO) has classified FGM/C into four different types: Type 1, removal of the clitoral glans; Type II, removal of the clitoral glans and labia minora; Type III, narrowing of the vaginal opening, which is known as infibulation; and Type IV, all other harmful non-medical modifications to the female genitalia.3 Women and girls who undergo FGM/C suffer from a spectrum of short- and long-term complications such as psychological trauma, menstrual problems and chronic infections depending on the type of FGM/C and conditions under which the procedure is performed.4
The prevalence of FGM/C varies between continents and countries, with the highest rates being reported in the African Region (AFR),5 with almost all women in Somalia, Guinea and Djibouti having undergone FGM/C.6–8 In high-resource settings, FGM/C is localised to migrant and refugee communities.9 10
Household surveys, such as Demographic and Health Surveys (DHS) and Multiple Indicator Cluster Surveys (MICS), provide the mainstay of data on FGM/C and allow progress towards the Sustainable Development Goals to be monitored across countries and regions.11 A better understanding of the risk factors and social determinants associated with FGM/C will enable key stakeholders and policymakers to better inform and strengthen programmatic interventions that aim to eliminate FGM/C. Thus, an understanding of these factors is essential to progress towards eliminating FGM/C and achieving SDG 5.3. This systematic review aimed to comprehensively examine the factors associated with FGM/C, including risk factors, protective factors and social determinants in different geographic regions and countries.
Methods
Search strategy
A systematic search of published articles was conducted in Medline, PsycInfo, Web of Science and Embase databases from inception to March 2020 with no language restrictions. In addition, searches of the grey literature were also conducted including reports of international non-governmental organisations and Google searches. The search was limited to include studies published between 2009 and 2020. The search terms included various synonyms of FGM/C such as ‘female genital cutting’, ‘female genital alteration’ and ‘female genital circumcision’. The search strategy is further detailed in online supplemental table 1. Duplicates were removed in EndNote and articles were imported to Distiller SR software.12 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guideline was followed.13
Supplemental material
Inclusion and exclusion criteria
This study was part of a systematic review on FGM/C that examined the prevalence and risk factors of FGM.14 Studies were included if they examined factors associated with FGM/C, had a case-series, cross-sectional, case-control or cohort design, and compared factors between women or girls with FGM/C to those without FGM/C. Factors examined in this systematic review correspond to risk factors, protective factors and social determinants of FGM/C. We excluded studies that did not report on factors associated with FGM/C using quantitative methods, studies that only presented perspectives or attitudes towards FGM/C, systematic reviews, conference proceedings and letters to editors. Where studies have used the same data source, the most recent publication was included in the review.
Definition of FGM/C
The outcome in this systematic review is FGM/C, which refers to all procedures that involve the total or partial removal of external female genitalia or other injuries to the female genital organs.3
Study selection
Two researchers independently screened the titles and abstracts of the articles to determine whether studies qualified for full-text review. At the full-text review stage, two researchers independently assessed the eligibility of studies for inclusion and stated the reasons for exclusion. Disagreements were reconciled through consulting a third reviewer as necessary.
Data extraction
Data were extracted by two reviewers using a tailored data extraction form on Distiller SR.12 Data from each study were extracted by one reviewer, which was verified by a second reviewer. Disagreements were addressed through discussion and with a third reviewer as necessary. Information extracted from each article included: author, publication year, year of data collection, the age range of the population or sample, study design, sample size, sampling method, country of origin, host country/region, FGM/C type, and risk or protective factor or social determinant of FGM/C. Factors were considered to be any variables that could have a plausible causal relationship with FGM/C. For each factor, the odds ratio (OR), risk ratio and 95% confidence interval (95% CI) were extracted for both unadjusted and adjusted analyses. If a study did not present a point estimate, the proportion in each category and the P-value were extracted.
Study quality assessment and risk of bias
The risk of bias of included studies was assessed using the Clarity Group assessment tool, McMaster University.15 16 Answers to the tool measures were either 'definitely yes' (low risk of bias), 'probably yes', 'probably no' or 'definitely no' (high risk of bias). We rated the studies as 'low risk of bias for all key domains', 'unclear risk of bias for one or more key domains' and 'high risk of bias for one or more key domains'. No study was excluded from this systematic review based on the methodological quality.
Data synthesis
Any variables considered to have a causal relationship with FGM/C were included in the data synthesis. A meta-analysis was not possible due to the large heterogeneity between studies. As a result, data from included studies were analysed using narrative synthesis. In particular, associated factors were grouped to reflect three different levels of the socio-ecological model (individual, parental/household and community levels). These were categorised into either protective factors or risk factors. Results from individual studies were further described according to age group (women or girls), country of origin, and WHO region (online supplemental table 2).
Public patient involvement
Ubah Ali, a co-author of this review, is a survivor of FGM and co-founder of Solace for Somaliland Girls, an organisation committed to eradicating all types of FGM across communities in Somaliland. She assisted in the interpretation of the data and drafting of the manuscript to ensure contextualisation of the findings.
Results
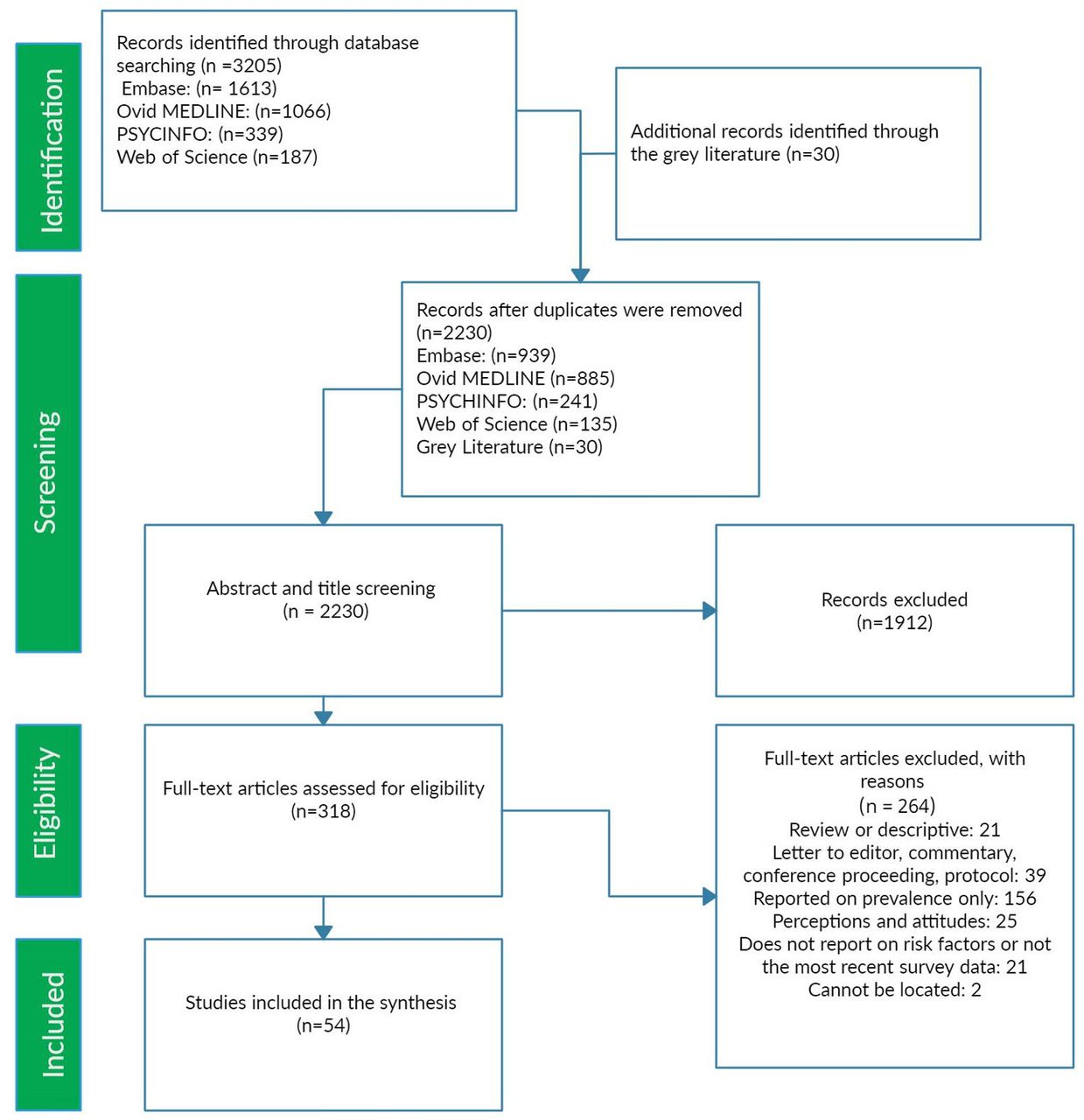
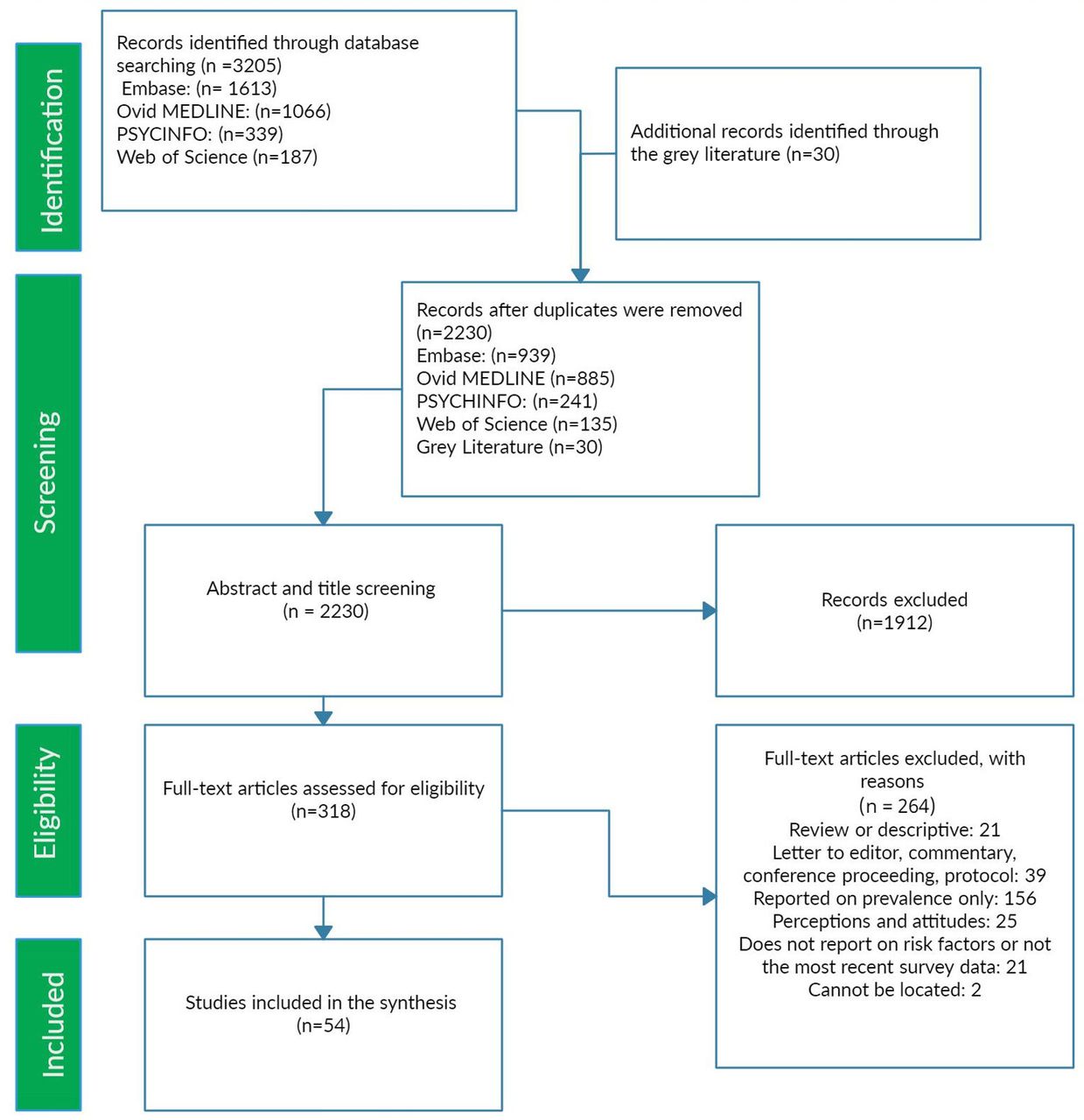
A total of 3205 records were retrieved from the databases and the grey literature. After duplicates were removed, 2230 abstracts were screened. A total of 318 articles were selected for full-text assessment, of which 54 were included in the final analysis (figure 1). Of those, 33 studies examined FGM/C status among women of reproductive age, 19 studies examined FGM/C in girls aged 0–15 years and two studies examined FGM/C in both the mother and daughter. In the latter two studies, data were presented for both women and daughters.17 18 Eight studies had overlapping age groups where the authors did not segregate results between women and girls. These studies were categorised into the most appropriate category as either women19–21 (table 1) or girls22–26 (table 2).
{kind=link}
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow chart of study selection.
Determinants of female genital mutilation/cutting (FGM/C) among girls and infants
Determinants of female genital mutilation/cutting (FGM/C) among women of reproductive age (15–49 years)
The main modality of data collection was household surveys (n=21), including seven studies that used MICS or DHS data, followed by hospitals or clinics (n=16), community-based studies (n=8), schools or universities (n=6) and databases or online survey (n=3). Most studies reported data on FGM/C based on participants’ or parents’ self-reporting (n=43) and 11 were based on physical examination. Only 22 studies reported on who performed FGM/C; among these, 16 showed that the procedure is most often carried out by a traditional practitioner (data not presented). Over half the studies were conducted in the AFR (n=29), followed by the eastern Mediterranean region (EMR) (n=18), European region (n=3), region of the Americas (n=3) and western Pacific region (WPR) (n=1). Seven studies described the determinants of FGM/C among migrants or refugees in high-resource settings.10 27–32 Sample sizes in the included articles ranged from 200 to 46 713, with 33 studies based on a sample size of fewer than 1000 women or girls. The range was smaller in migrant studies from 23 to 2173 women. All studies were cross-sectional except four studies that utilised a case-control design.10 19 33 34 Characteristics of all included studies are described in online supplemental table 2.
Across all studies, there were 34 determinants identified, which were either protective or risk factors for FGM/C. The most common determinants reported among women and girls are summarised in tables 1 and 2, respectively, and include being a Muslim (n=24), mother’s level of education (n=24 studies) and area of residence (urban or rural) (n=23). A detailed description of the association of these factors with FGM/C status (results by study) is available in online supplemental table 3. Other less common factors are described in online supplemental table 4.
Risk of bias
Overall, eight articles showed a low risk of bias,26 35–41 20 articles had a high risk of bias10 21 24 25 27 30–32 34 42–52 and 26 articles demonstrated an unclear risk of bias.17–20 22 23 28 29 33 53–69
Factors associated with FGM/C
Individual characteristics
Wealth
The association between wealth and FGM/C was examined in 10 studies conducted among women of reproductive age17 18 29 34 37 40 51 54 67 68 and eight in girls.17 18 22 38 39 59 64 66 Overall, 9 66 of 18 studies showed little to no influence for wealth on the FGM/C status of women and girls.18 22 29 38 39 54 64 66 68 Three of 10 studies showed that being in a higher wealth quintile was protective against FGM/C among women of reproductive age17 34 51 and two of eight studies showed that an increase in household wealth decreased the likelihood of having a daughter subjected to FGM/C.17 59
Religion
Twenty-four studies assessed the association between being Muslim and FGM/C status among women (n=15) and girls (n=9).18 19 22 23 27 28 30 31 35 36 39–41 46 51 54 57–59 61–63 66 68 Overall, 15 studies found a significant positive association between being Muslim and FGM/C status18 19 22 27 28 30 31 35 36 39 40 57–59 61 and nine found no significant relationship.23 41 46 51 54 62 63 66 68 These results were context specific. In addition, a study in Iran found that Sunni Muslim women were more likely to have FGM/C than Shi’a Muslim women .60(see tables 1 and 2)
Parental characteristics
Mother’s age
Nine studies examined the association between mother’s age and daughter’s FGM/C status.17 35 38 39 45 55 59 64 Daughters of mothers of older age were more likely to have FGM/C in four of nine studies.17 35 38 45 Among a pooled sample of six DHS surveys from Nigeria, Egypt, Mali, Kenya, Guinea and Burkina Faso, the age of the mother did not have a statistically significant association with FGM/C.59
Maternal education
Seven studies assessed the influence of the level of maternal education on FGM/C among women of reproductive age.20 36 51 52 54 56 61 A higher level of maternal education was protective against FGM/C, particularly among women whose mothers had attained primary level education compared with uneducated women,20 36 51 were literate versus illiterate56 or had reached secondary level schooling and above compared with primary education or no education.61
Seventeen studies assessed the influence of the mother’s level of education on FGM/C among girls and daughters.17 22–26 35 38 39 44 45 55 57 59 64 66 69 Fourteen out of seventenn studies showed that increased maternal education, in particular, being literate versus illiterate,38 55 and having a secondary or higher level of education17 23 25 26 35 44 59 69 decreased the likelihood of FGM/C among daughters. All 17 studies were either conducted in the AFR (13 studies) or the EMR (4 studies). Higher levels of maternal education decreased the likelihood of daughter’s FGM/C in three of four studies conducted in the EMR17 26 44 and 11 of 13 studies conducted in the AFR.22–25 35 38 45 55 57 59 69
Paternal education
Higher paternal education was protective against FGM/C in three of five studies conducted among women of reproductive age,20 52 56 while two studies showed no association between paternal education and FGM/C.51 54 All five studies were conducted in the EMR.20 51 52 54 56 Six of 10 studies conducted among daughters demonstrated that the risk of FGM/C decreases with increased level of paternal education.23 25 44 45 55 69 One of the four studies, which showed no statistically significant relationship, examined FGM/C among infants46 rather than adolescents or young children.
Parents’ occupational status and employment
The relationship between having a mother who is a professional or an employee was examined in nine studies and was found to be protective in one study,50 a risk factor in one57 and not statistically significant in seven studies.23 25 38 39 44 59 64 In two studies, the relationship was statistically significant at the unadjusted level but was no longer statistically significant after adjusting for confounders.23 44
One of four studies showed that an employed fathers had a lower prevalence of FGM/C among daughters than unemployed fathers,25 and the relationship was not statistically significant in three studies.23 44 64
Family history of FGM/C
Ten studies examined whether a family history of FGM/C affected the likelihood of FGM.17 35 37 39 44 51 52 59 60 66 In particular, nine studies investigated the relationship between the FGM/C status of girls based on whether their mothers had FGM/C.17 35 37 39 51 52 59 60 66 Having a mother with FGM/C led to higher odds of a daughter(s) having FGM/C in seven of nine studies.17 35 37 51 52 59 60 The relationship was especially strong in Iraq (Kurdistan) (adjusted OR (AOR) 15.1, 95% CI 10.6 to 21.6)),52 Eritrea (AOR 8.59, 95% CI 5.63 to 13.10),35 Egypt (Sohag and Qena) (AOR 9.12, 95% CI 2.11 to 14.09)51 and Yemen (AOR 7.40, 95% CI 6.01 to 9.13).17 Having a family member such as a sister or a grandmother subjected to FGM/C significantly increased the likelihood of being subjected to FGM/C in all three studies reporting FGM/C family history.44 51 60
Community-level determinants
Urban versus rural region
Twenty-three studies examined whether FGM/C status differed between urban and rural areas.18–20 22 23 33 36–42 44 46 49 51 54–56 58 59 61 Of the 23 studies, 13 showed that women living in urban areas were less likely to be subjected to FGM/C,44 seven studies did not show a statistically significant association22 37 39 41 42 44 46 and three studies showed that living in an urban area increased the likelihood of FGM/C.18 19 40 In a study based in Somalia, daughters of women residing in an urban area were 70% less likely to have FGM/C.38 Living in a rural area was one of the most influential sociodemographic characteristics affecting FGM/C among a sample of young women in Egypt (OR 8.2).51 Conversely, among Kenyan girls (aged 0–14 years) there was no statistically significant difference of FGM/C by place of residence.39
FGM/C as a religious requirement
Four studies examined the association between FGM/C and its practice on religious grounds among girls22 25 39 and among women aged 15–24 years.61 All four studies were conducted in the AFR, and three of these studies found a statistically significant association.22 25 61
Other risk factors identified from the literature
Several other determinants were reported in the studies. Mothers who had a positive attitude towards FGM/C continuation were more likely to have a daughter subjected to FGM/C in three of four studies.17 38 39 Girls whose mothers had lower knowledge of FGM/C complications were more likely to be subjected to this practice in one of three studies.25 The participation of parents in anti-FGM/C activities was associated with a lower likelihood of FGM/C for their daughters in both studies.55 65 Some determinants were only examined in one study and showed a positive association with FGM/C such as mother’s underage marriage,17 high village FGM/C rate,22 cultural influence to perform FGM/C or community acceptance55 or being an undocumented migrant.28 There was no statistically significant association between FGM/C status and women’s decision-making ability,59 women’s ownership of land39 and domestic abuse39 (online supplemental table 4).
Discussion
This study showed that there was a wide variety of determinants for FGM/C at the individual, familial, community and structural levels. Parental education and living in an urban area appeared to have protective effects against FGM/C for both women and girls in the majority of studies. For both women and girls, the majority of studies showed that being a Muslim, perceiving that FGM/C has religious grounds, and having a family history of FGM/C were risk factors for FGM/C. Furthermore, proxy factors related to women’s status in society appeared to be related to FGM/C, such as underage marriage and education.
FGM/C is a harmful practice that removes healthy female genital tissue causing short- and long-term impacts on the health and well-being of women.70 Furthermore, the practice violates the human rights of women and girls and is an extreme form of discrimination.71 In addition to the individual and societal impacts, the estimated economic cost of FGM/C due to obstetric, gynaecological, mental and sexual complications amounts to US$1.4 billion every year.72
Results in context
FGM/C is a result of interrelated and complex factors associated with gender norms; this review showed that the literature focused on determinants at the micro and meso levels, and data were scarce on the impact of social norms on FGM/C. Social norms are unhidden rules among community members that guide behaviour by setting a perception of rewards, benefits or punishment.73 Furthermore, women and girls have a social obligation to continue with FGM/C, and deciding to stop the practice places women and girls at risk of shame, stigmatisation, exclusion and rejection from their communities.71
This study demonstrated that the majority of studies that examined rurality or family history of FGM/C showed they were risk factors for FGM/C; these variables may be proxy indicators for social norms. A systematic review examining men’s attitudes, beliefs and behaviours regarding FGM/C demonstrated mixed perceptions about the practice as some men wished to abandon the practice but others considered it a social obligation.74 An enabling environment to support the discontinuation of FGM/C demands enhancing the men’s role, whether the husbands, fathers or community leaders, as promoters who can partner to break this social convention.71 Qualitative studies report that women believe FGM/C is a religious obligation.75 76 Narratives and experiences of communities that practise FGM/C suggest that FGM/C is a ritual or tradition that has been a social and cultural norm across generations and is a requirement for marriage.76 77
This review found that the majority of studies identified urban status as protective against FGM/C among women. Although some urbanised cities are lagging in achieving gender equality goals, there appears to be an association between urbanisation and women’s ability to make strategic life choices.78 One reason for this relationship is that urbanisation improves women’s educational participation and empowers them economically and politically.79 The relationship between residence in urban areas and female schooling may explain how urbanisation contributes to better gender equality and well-being for women.78 ,43
This systematic review showed that the majority of studies assessing parental education found that it was protective against FGM/C for women and girls. This finding is supported by the literature; Link and Phelan argue that female education is one of the main proxy variables for autonomy and that it plays a role in preventing violent outcomes.80 The demonstrated association between education and FGM/C may be a reflection of the effect of education on improving the interpersonal skills of women and girls, their social status and cultural outlook, and their ability to lead independent lives and oppose gender roles and traditions.81
There were several factors related to women’s status in society that were shown to be risk factors for FGM/C, including low maternal education status, child marriage, being an undocumented migrant, and living in a village with high FGM/C rates. Progress towards gender equality through women’s inclusion in the workplace and education may be a pathway to ending FGM/C.82 Furthermore, the United Nations General Assembly stated in a resolution that member states should “pursue a comprehensive, culturally sensitive, systematic approach that incorporates a social perspective and is based on human rights and gender equality principles in providing education and training to families, local community leaders and members of all professions relevant to the protection and empowerment of women and girls to increase awareness of and commitment to the elimination of female genital mutilations” (United Nations, 2012; UNFPA, pp. 3–4).83 The pursuit of gender equality, women’s empowerment, and elimination of FGM/C is cross-cutting, and requires engagement at all levels of the socio-ecological model to meet the Sustainable Development Goals.
Strengths and limitations
This review used rigorous search strategies and standardised systematic review methodology to ensure the inclusion of all eligible studies and the accurate synthesis of these studies. This review had several limitations; approximately half of the studies had a high risk of bias. In addition, many studies were cross-sectional, so reverse causality cannot be excluded for many determinants in the included studies. Furthermore, there was considerable heterogeneity between studies due to the broad range of study locations, participants and methods to assess and categorise the various determinants.
This review only presented factors associated with FGM/C as presented in the literature and there may be other related factors that were not reported in the included studies. For example, the commercial or economic determinants of FGM/C, where traditional practitioners perform FGM/C for financial reasons, perpetuating the practice in communities.84
Recommendations for future research
The present research mainly demonstrates evidence on FGM/C determinants from resource-poor settings, leaving gaps in knowledge related to migrant health in high-income countries. Further work should be completed to understand the effectiveness of policies and interventions that aim to eradicate FGM/C. An evaluation of “grassroots” and community-level interventions or policies will allow an understanding of the barriers and facilitators to implementation, and the potential to extrapolate these interventions and policies to other communities.
Conclusions
This review identified factors related to FGM/C, which include lower parental education, religion, rural residence, and family history of FGM/C. Disrupting the intergenerational trauma of FGM/C through education, advocacy, and changing social norms may be potential pathways to eliminating FGM/C. Gender equality, improving women’s status in society, and education of girls are cross-cutting Sustainable Development Goals that will improve the health and well-being of women globally. Approaching women’s status in society holistically is vital to tackling harmful practices against women.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
We would like to acknowledge the assistance of Ms. Sandra Kahwaji and Ms. Jana Abu Ayash for their help in the title and abstract screening of articles. We thank Dr. Sawsan Abdulrahim for insightful comments and edits on preliminary drafts.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
ZE-D and LF contributed equally.
Correction notice This article has been corrected since it was first published. Under the section about data extraction, the first two sentences have been modified.
Contributors SM conceived the study and CAkl and CAkik contributed to the study design. SM and LF wrote the protocol with contributions from CAkl and CAkik. ZD completed the literature search. LF and ZD selected the studies and extracted relevant data. ZD analysed the data and wrote the first draft of the paper. SM supervised ZD. SM, CAkl, CAkik, UA and ZD revised drafts and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.