Article Text

Statistics from Altmetric.com
Dear Editor,
Overall levels of childbearing are significantly higher in England and Wales (total fertility rate of 1.62 and 1.49, respectively, in 2021) than in Scotland (1.31), but few studies have investigated the role of abortion or contraception as proximate determinants of fertility, leaving a key gap in knowledge. This is largely due to a paucity of continuously collected comparable data, since surveys that have historically collected such data (ie, the Omnibus Survey, General Household/Lifestyle Survey) have been discontinued. Existing administrative data on abortion rates collected from 2009 to 2020 show that abortion rates are consistently lower in Scotland than in England and Wales—by approximately eight abortions per 1000 women per year—meaning use of abortion cannot account for the persistently lower fertility levels in Scotland. Our analysis thus focuses on contraception and is the first to identify and quantify the extent of cross-national differences in Britain in contraceptive use, as well as method mix. The mix of contraceptive methods used is important because methods vary in their effectiveness at preventing pregnancy1 and may thus influence fertility.
We analysed data from the National Surveys of Sexual Attitudes and Lifestyles (NATSAL-1 to -3, 1990, 2000 and 2010). The more recent interim surveys (NATSAL-COVID-19 surveys 1 and 2) did not ask about contraception in the same way and do not permit cross national analysis due to smaller sample sizes.2 We pooled data from the three available surveys for respondents aged 16–49 years who had ever had heterosexual intercourse (n=35 245), using weights provided by NATSAL. Respondents were presented with a list of contraceptive methods and asked, ‘Which have you used at all with a partner in the past year?’. We defined long-acting reversible contraception (LARC) as implants, intrauterine systems, intrauterine devices, and injectables. Implants and intrauterine systems were introduced after 1990 so are not accounted for in NATSAL-1. If a respondent reported having used multiple methods in the past year, we identified the most effective method. Multinomial logistic regression was used to model country differences in use of contraception, by method type, with outcome variable categories ‘no method used’ (the reference outcome), ‘barrier/traditional method’, ‘pills or patch’, ‘LARC’, ‘female sterilisation’, and ‘male sterilisation’.
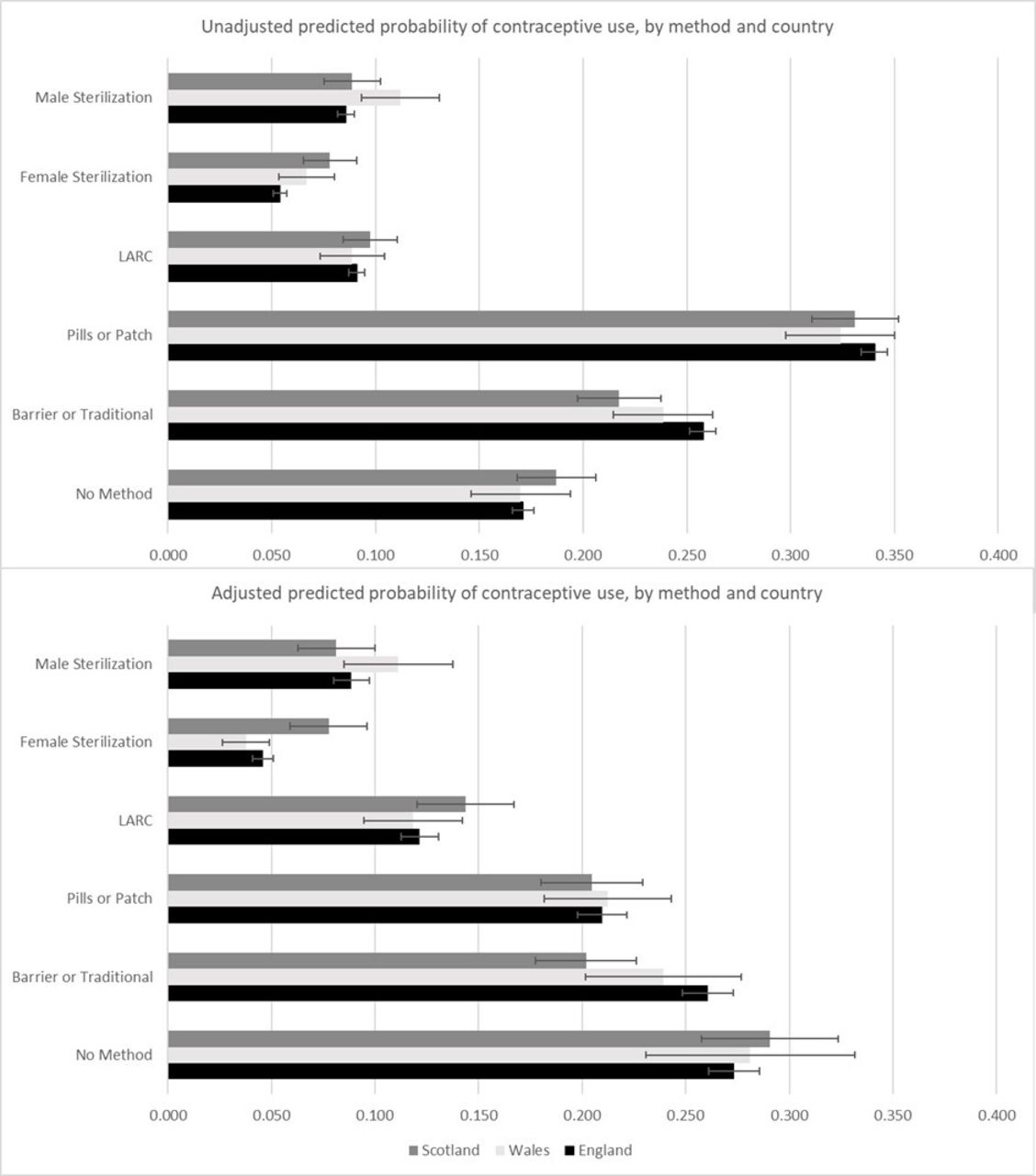
Figure 1 shows the unadjusted and adjusted predicted probabilities of contraceptive use, by country and method type. Controls used in the adjusted predicted probabilities include survey year, age, parity, partnership status, education, religiosity, ethnicity, and sex. Method mix differed notably across countries, with significantly greater levels of female sterilisation use in Scotland as compared with England, and significantly lower levels of barrier/traditional method use, which is especially pertinent because they are among the most and least effective methods, respectively. These differences persisted in the adjusted model, indicating that differences in the population composition of England and Scotland (ie, a larger share of ethnic minority groups in England) do not account for the countries’ method variation. In contrast, male sterilisation had a higher likelihood of use in Wales compared with England, but the difference disappeared in the adjusted model.
{kind=link}
Predicted probabilities from multinomial logistic model of contraceptive use using NATSAL surveys 1990–2010, sexually active men and women aged 16–49 years. Baseline outcome is ‘no method used’. Adjustments: survey year, age, parity, partnership status, education, religiosity, ethnicity, and sex. LARC, long-acting reversible contraception; NATSAL, National Surveys of Sexual Attitudes and Lifestyles.
Using estimates of contraceptive effectiveness (ie, how many unintended births would occur to 100 women using a certain contraceptive method, given typical use)1 and the method mix for each country, we calculated the predicted number of births per 1000 sexually active women. For example, the difference in estimated births between England (279 births) and Scotland (243 births) for women in their 30s based on the 2010 method mix was 36 births per 1000 sexually active women. For perspective, the actual fertility rates had a gap of around 10 births per 1000 women. Although contraceptive use alone cannot predict fertility rates because other factors also influence fertility, we found the country differences in method mix effectiveness were strong enough to translate potentially to meaningful differences in predicted number of births. New survey data are needed to investigate further the most recent contraceptive use patterns, which the postponed NATSAL-4 will provide once it becomes available.
Ethics statements
Patient consent for publication
Acknowledgments
This research was supported by Economic and Social Research Council grant ES/S009477/1 (Understanding Recent Fertility Trends in the UK and Improving Methodologies for Fertility Forecasting)
Footnotes
Twitter @bkuang1769
Contributors BK planned the study, conducted the data analysis and drafted the manuscript. AB planned the study and provided editorial support on the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.