Article Text

Abstract
Objective Fear of pain during intrauterine device (IUD) insertion can be a barrier to widespread use of this safe and highly effective contraceptive method. Our objective was to determine the effectiveness of topical 10% lidocaine spray for pain control during IUD insertion.
Methods A total of 200 subjects with the request for IUD insertion were included in the study. The patients were randomly divided into two groups: lidocaine spray (n=100) and placebo (n=100). The pain experienced during the procedure was measured immediately after insertion by a standard Visual Analogue Scale (VAS) administered by a separate researcher with maintenance of allocation concealment.
Results The mean pain score during the procedure was 1.01±1.20 in the lidocaine spray group and 3.23±1.60 in the placebo spray group (p<0.001). Lidocaine spray treatment significantly lowered the overall procedural pain score compared with placebo.
Conclusions Significant pain reduction during IUD insertion can be achieved by using 10% lidocaine spray alone. Lidocaine spray can be accepted as a non-invasive, easy to apply and more comfortable local anaesthetic method for IUD insertion.
Trial registration number NCT02020551.
- intrauterine devices
- pain relief
- lidocaine
Statistics from Altmetric.com
Key message points
Effective pain relief during intrauterine device (IUD) insertion can be achieved by the use of 10% lidocaine spray.
Lidocaine spray can be accepted as a non-invasive, easy to apply and more comfortable local anaesthetic method.
Strategies designed to reduce insertion-related pain have great public health importance considering the large numbers of women who undergo IUD insertion.
Introduction
The intrauterine device (IUD) is a highly effective contraceptive method equal in efficacy to tubal sterilisation and associated with lower rates of discontinuation when compared to other reversible methods.1 ,2 The IUD is used by approximately 15% of reproductive-aged women in developing countries and 8% in developed countries.3
The IUD insertion procedure is associated with pain and discomfort in several ways: application of the tenaculum to grasp the cervix as well as transcervical actions including measuring uterine depth, inserting the uterine sound, inserting the IUD in the inserter tube through the cervix, and irritation of the endometrial cavity with the device.4 ,5 Because of concern about causing procedural pain, the majority of health care providers selectively use or recommend less effective contraceptive methods.6 ,7 Various types of pain control methods have been proposed, including nonsteroidal anti-inflammatory drugs (NSAIDs), anxiolytics and local cervical anaesthetics in the form of intracervical gels, cervical and paracervical blocks, and cervical ripening agents such as misoprostol.5 ,8–14 Most women experience mild to moderate pain during IUD insertion. Sometimes the pain is severe and can be associated with vasovagal reactions such as lightheadedness, nausea, pulse rate alterations, or even syncope and convulsions.4 ,15 Strategies designed to reduce insertion-related pain have great importance in public health, considering the large number of women who undergo IUD insertion. Therefore, it is important to identify a safe, effective and easy-to-apply method of analgesia during IUD insertion. In a Cochrane Review evaluating interventions for pain during insertion, one poorly designed study suggested that topical 2% lidocaine gel may reduce insertion-related pain and warranted further investigation.16
Lidocaine in spray form is a simple and convenient local anaesthetic with minimal adverse effects and is often used in dentistry for oral mucosal anaesthesia during minor surgical interventions. The spray form may provide easy application and better patient acceptance than other forms of lidocaine administration. However, there is no evidence regarding the effectiveness of its use in pain control during IUD insertion. To the best of our knowledge, the present study, in which lidocaine spray was used as a pain control method during IUD insertion, is the first such research reported in the literature.
Methods
Study design
A randomised, double-blind, placebo-controlled trial was designed and carried out at our tertiary centre's family planning clinic from December 2013 to January 2014. Approximately 3200 women attend our family planning department each year for IUD insertion. The treatment and control groups consisted of parous women aged 19–49 years and requesting IUD (Copper-T380A) insertion for contraception. All patients had been delivered vaginally. No nulliparous women were included in the study as very few such women use IUDs in our country. Inclusion criteria for this study were: (1) aged 18 years or more; (2) accepting IUD as the method of contraception; (3) no known previous allergic reaction or sensitivity to lidocaine or placebo spray; (4) no accompanying extraordinary medical or surgical conditions necessitating special attention; (5) no specific request for anaesthesia, or suspected pathology necessitating anaesthesia; and (6) no history of chronic pelvic pain or dysmenorrhoea. Exclusion criteria were: (1) currently pregnant or within 2 weeks of conclusion of a pregnancy; (2) presence of a known uterine anomaly or fibroid distorting the uterine cavity; (3) contraindication to a copper IUD based on Centers for Disease Control medical eligibility criteria; (4) untreated acute cervicitis or pelvic inflammatory disease; (5) known cervical stenosis or extraordinary surgical conditions necessitating cervical dilators; (6) any systemic diseases or medications that would affect the perception of pain; (7) current or past history of illegal drug or narcotic use; (8) inability to understand how to score a 10-cm visual analogue scale (VAS) for pain; and (9) a VAS pain score other than 0 (no pain) just before IUD insertion. With these exclusion criteria we aimed to achieve a homogeneous study population. Included participants were scheduled for IUD insertion, and none of the participants had received medication such as analgesics or misoprostol for the 7 days prior to the procedure.
The primary outcome for this study was the IUD insertion pain score, as measured by the 10-cm VAS. To determine sample size, reference values [means, standard deviations (SDs) and reference sample sizes] were taken from a study conducted by Li et al.17 Assuming a reduction of pain by 0.5 SDs was acceptable, it was estimated that at least 95 subjects were required in each study arm to detect a clinically significant difference between the two groups on a 10-cm VAS scale when assuming a power of 80% to detect the primary hypothesis and a type I error of 0.05. Assuming a 5% dropout rate, we planned to recruit a total of 200 women (up to 100 subjects per study arm). Analyses were made by G*Power 3.1.7 (Heinrich Heine University, Düsseldorf, Germany).
The participants completed an enrolment questionnaire so that we could assess sociodemographic characteristics and medical information. Medical variables included parity, lactation status, previous contraceptive use, last menstrual period, date of last pregnancy, mode of past deliveries, and an obstetric and gynaecological history. Study participants were randomly assigned to one of two groups. A computer-generated random number chart (IBM SPSS Statistics for Windows V.20.0; IBM Corp., Armonk, NY, USA) was used for group randomisation. The treatment arm consisted of 100 participants receiving four pumps (net 40 mg) of 10% lidocaine spray (Xylocaine® 10% pump spray, 10 mg/ml, Astra Zeneca) for topical anaesthesia, and the placebo arm consisted of 100 participants receiving four pumps of isotonic saline solution spray (see online-only Supplementary Material Figure 1).
Each patient underwent a pelvic examination along with transvaginal ultrasound to confirm the uterine shape and size as well as to exclude any other pelvic pathology. Each of the 200 consecutive patient numbers was written on an opaque yellow envelope while the assignment code was written on a separate paper that was then sealed inside. At the time of IUD insertion, the responsible nurse opened the envelope to reveal the assignment, and she prepared the trial medications accordingly. Of two identical spray bottles wrapped in black paper, one contained 10% lidocaine and the other normal saline. Sprays were indistinguishable in appearance, colour and consistency. The patients, the anaesthesia technician performing VAS, and the gynaecologist performing the procedure were blinded to the contents of the bottles.
No cervical ripening agents were used. We administered three puffs to the cervical surface and one puff specifically towards the external cervical os and waited for 3 minutes (as suggested by the manufacturer) to allow the anaesthetic to take effect. After the application, the cervix was grasped with a tenaculum and straightened to the uterine axis, and the IUD was inserted in the standard manner after sounding of the uterus. Preparation for IUD insertion was performed according to the clinic's description: in the lithotomy position, a water-lubricated, single-use speculum was introduced, and the vagina and cervix were cleansed using standard povidone iodine solution. Insertion was completed next: the uterine depth was measured using a metal sound, and the IUD was inserted using the withdrawal method. Patients were observed for 30 minutes after the procedure.
Patients were asked to rate their pain level on a standard continuous 10-cm VAS to quantify the pain, from 0 cm (no pain) to 10 cm (the worst pain ever). Pain scoring was first performed immediately before speculum placement (t1) and again immediately following insertion (t2). All procedures were performed by the same gynaecologist and team to avoid possible operator-dependent pain factors and other confounding variables.
Statistics
Normality was tested using the Shapiro-Wilk test. Variance homogeneity was tested using Levene's test. Values are expressed as mean±SD or median (25th to 75th percentile). Parametric comparisons were made using t-tests, non-parametric comparisons were made using the Mann–Whitney U-test. The PASW Statistics 18 programme (IBM Corp., Armonk, NY, USA) was used for all comparisons. Statistical significance was recognised when p<0.05.
Ethics approval
The study protocol was approved by the local ethics committee of Erciyes University. All participants who met the eligibility criteria were informed of the procedure and gave their informed written consent for study participation by the same doctor who performed the procedures. The study was performed in accordance with the Helsinki Declaration of the World Medical Association.
Results
A total of 223 patients were evaluated for eligibility. Twenty-three patients were excluded: five who refused to participate in the study and 18 who did not meet inclusion criteria (two had cervical stenosis, three had current analgesic use, five had acute cervicitis, one had a history of cervical conisation, and seven had histories of dysmenorrhoea or chronic pelvic pain). All procedures were successfully completed without severe complications or serious adverse reactions. There were five mild complications associated with vasovagal reaction such as nausea, vomiting and dizziness, but for which no treatment was needed. Of these, two were in the control group. Systemic side effects associated with 10% lidocaine spray were not observed. No statistically significant difference was found between the groups in terms of mean age, body mass index, gravidity or parity (Table 1). In addition, no difference was found in total procedure time from speculum insertion to speculum removal, which averaged 4 minutes.
Patient characteristics and pain scores
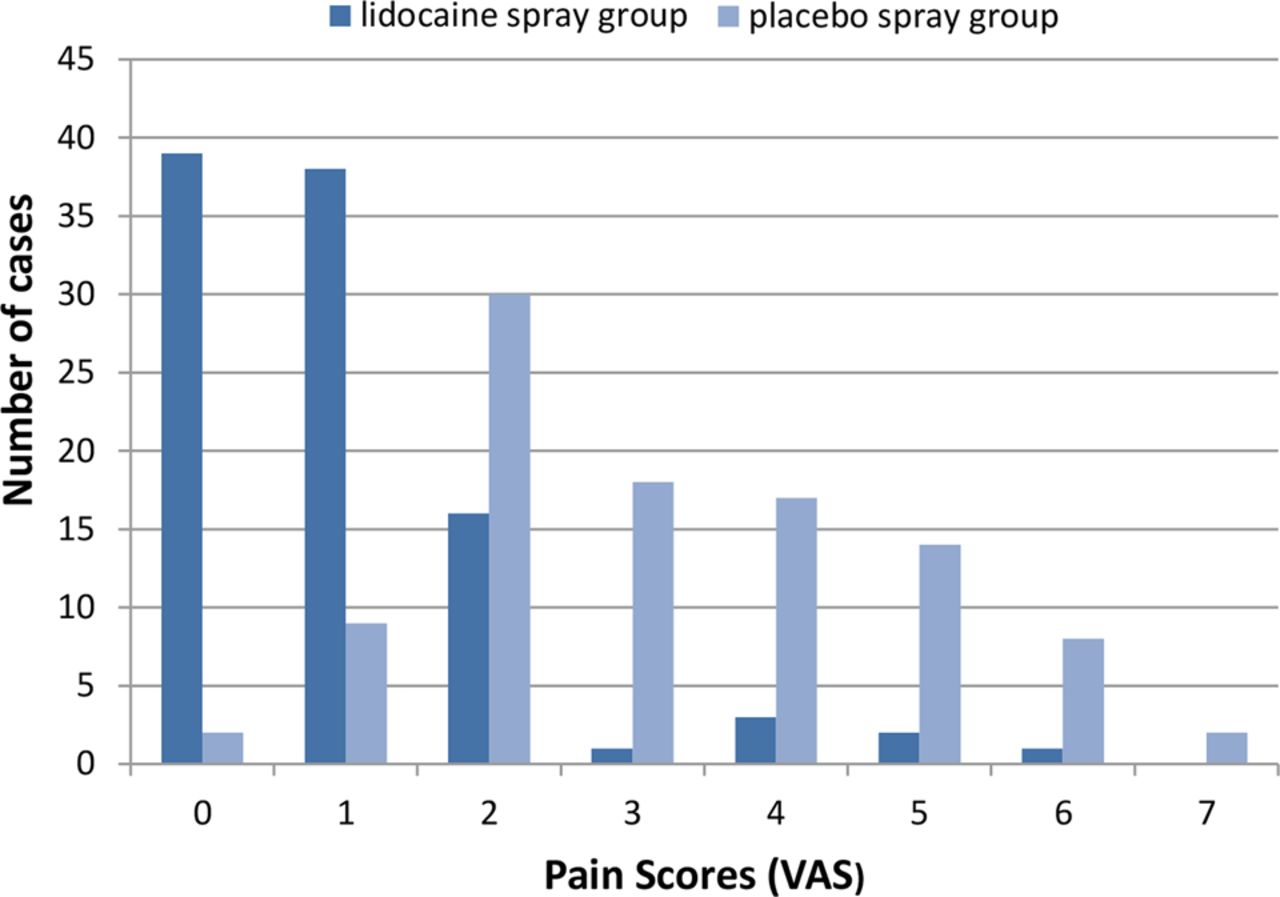
Procedural pain scores are illustrated in Table 2. Patients in the control group experienced greater pain than those in the treatment group (mean scores 3.23±1.60 vs 1.01±1.20, p<0.001). The number of patients who scored 4 and above within each group was evaluated. The frequency difference between groups was statistically significant (41% in controls vs 6% in the treatment group, p<0.001; Table 2).
Comparison of procedural pain scores
Pain score distribution in each group is presented in Figure 1. A significantly lower score for overall pain during the procedure was found in the treatment group compared to controls (p<0.001).

{kind=link}
Distribution of pain scores in each group. VAS, Visual Analogue Scale.
Discussion
Pain in minor surgical procedures has always been a problem in gynaecology. IUD insertion pain is important as this is one minor gynaecological procedure that is offered to millions of women worldwide. Thus, better pain control during this procedure could lead to more widespread IUD use, decreasing unintended pregnancies and their consequences because it is a safe, highly effective, long-term, reversible means of contraception.18
Many patients continue to find IUD insertion extremely painful and uncomfortable. In a prospective study by Marions et al.15 it was found that the majority (89%) of women reported moderate or severe pain during IUD insertion. Systemic premedication with NSAIDs and pre-procedural administration of misoprostol, paracervical block, anxiolytics, and local cervical anaesthetics in the form of intracervical gels have been studied for prevention of insertion-related pain.5 ,8–14 A Cochrane Review evaluating pain interventions during insertion concluded that no interventions had been properly evaluated.4 Only one trial investigated the effectiveness of 2% lidocaine gel, and this demonstrated a positive effect.16 However the Cochrane Review found that this study had limitations such as a faulty randomisation scheme, lack of proper sample size calculations, lack of proper blinding, and lack of allocation concealment. A recent study by Goldthwaite et al. compared lidocaine injection and lidocaine gel for tenaculum application and found that the injection was more effective. The VAS scores in both groups were low, and without a placebo group it was unclear whether there was any specific effect from the gel.19
Several clinical studies investigating the effectiveness of topical anaesthetics for IUD insertion-related pain control have been conducted.13 ,14 ,20 ,21 In these studies, only lidocaine HCl in gel form was used as a topical anaesthetic. To our knowledge, ours is the first randomised, double-blind, placebo-controlled trial of local lidocaine spray for pain control during IUD insertion. Lidocaine spray is a simple and convenient topical anaesthetic with minimal adverse effects. However, to date there is no evidence regarding its effectiveness in pain control during IUD insertion. We have shown that it is effective in reducing pain scores during IUD insertion. This finding is inconsistent with several other studies that examined the potential role of other forms of topical lidocaine for pain control during IUD insertion. Topical analgesics have been suggested for patient comfort, increasing the overall success of pain control during minor surgical gynaecological operations. Intrauterine lidocaine gel application, intrauterine lidocaine solution and transcervical lidocaine applications have been proposed.20–23
Lidocaine spray has been studied during other gynaecological procedures, with consistently positive results.24–27 Karasahin et al.24 ,25 showed that 10% lidocaine spray safely decreases perceived pain during first-trimester surgical abortion and hysterosalpingography. In agreement with both Karasahin et al.24 ,25 and Soriano et al.,26 we demonstrated a significant reduction in overall procedural pain in the lidocaine spray group compared with the placebo group.
The median pain score during IUD insertion among women in the placebo group in Allen et al.'s28 study was 3.6 cm. In our study it was 3 cm. However, the pain scores in our study were lower than those reported for IUD insertion in Maguire’s, McNicholas’ or Allen's studies.13 ,21 ,28 This discrepancy may be related to cultural and personal differences in pain perception between the populations studied since pain is deeply influenced by culture, personal experiences and pain tolerance.
There are some limitations to our study. Ideally, it would have had three arms: a lidocaine spray arm, a placebo spray arm, and a no treatment arm. Secondly, in this study, pain was not measured at the various stages of IUD insertion. An additional assessment of pain 10 minutes after insertion would have been useful in evaluating the moderately delayed prostaglandin-related cramping pain that many women experience. However, assessment of the relatively immediate somatic pain – probably largely tenaculum-related and quite variable between women – was valuable, because this is intuitively the primary pain that lidocaine spray might be expected to reduce. Finally, another possible weakness of our study is the lack of nulliparous women. This is a reflection of the population of women who presented for care at our family planning centre.
Conclusions
Our study demonstrated that lidocaine spray can be effective in control of procedure-related pain during IUD insertion when compared with placebo. More larger-scale, prospective and homogeneous studies involving topical anaesthetics or other interventions are needed to determine the effectiveness, safety and optimal dosage of lidocaine spray.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Twitter Follow Sezin Ozyurt at @sezinsaygi
Competing interests None.
Ethics approval Erciyes University Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue