Article Text

Abstract
Background Endometriosis is a chronic and progressive condition of women of reproductive age. It is strongly associated with significant impairment of sexual function.
Aim To objectively evaluate the impact of laparoscopic excision of endometriosis on sexual function in patients with deep infiltrating endometriosis (DIE) compared to healthy women.
Setting and design Prospective study, including 250 patients with a diagnosis of DIE scheduled for laparoscopic surgery and 250 healthy women.
Methods A sexual activity questionnaire, SHOW-Q (Sexual Health Outcomes in Women Questionnaire), was used to collect data pertaining to women's satisfaction, orgasm, desire and pelvic problem interference with sexual function. Women with DIE underwent complete excision of endometriotic lesions. All participants were asked to complete the SHOW-Q questionnaire before and after surgery.
Results SHOW-Q scores in the endometriosis group before and 6 months after surgery were compared with the healthy group scores. A significant improvement was found between pre- and post-treatment in the scores of the satisfaction scale, desire scale and pelvic problem interference scale of SHOW-Q. The distribution of post-surgery SHOW-Q scores was comparable to healthy women's scores apart from the orgasm scale score, which was unchanged in the post-surgery group.
Conclusions The surgical approach to treatment has a positive impact not only on organ impairment but also on sexual function in women affected by DIE.
- endometriosis
- oral contraceptives
- infertility
- natural family planning
- general practice
- counselling
Statistics from Altmetric.com
Key message points
Deep infiltrating endometriosis (DIE) is associated with a significant reduction of sexual function. This generally improves with surgical treatment.
In a sexual function questionnaire, satisfaction, desire and pelvic problem interference scores were significantly improved after surgical treatment.
Following surgery, sexual function of women affected by DIE is generally comparable to that of healthy women.
Introduction
Endometriosis is a chronic condition affecting women of reproductive age. It is characterised by the presence of endometrial-like tissue outside the uterus, which induces a local inflammatory response.1 The condition affects 5–10% of women of reproductive age2 who typically present with pelvic pain and infertility.
Deep infiltrating endometriosis (DIE) is defined as a form of endometriosis that penetrates more than 5 mm under the peritoneal surface.3 It is widely accepted that endometriosis, particularly DIE, is associated with a significant reduction of quality of life and sexual function.4–6 Many factors may contribute to altering sexual function in women with DIE: pain, tissue fibrosis, the chronic inflammatory status and the presence of neuroactive agents.7 ,8
As endometriosis is a benign disorder, the main goal of treatment should be to alleviate pain and improve symptoms. Conservative measures, including medical therapy, could be safe and harmless but they are often ineffective, especially in DIE.9 Surgery for symptomatic endometriosis is generally satisfactory with a low recurrence rate, provided that complete removal of the endometriotic deposits has been achieved.10 However, laparoscopic management of DIE is a complex surgical procedure, which may be complicated by urinary or intestinal neurogenic impairment,11–13 especially in cases where nerve-sparing surgery is not feasible.12
In this prospective study we objectively evaluated the impact of laparoscopic excision of endometriosis on sexual function in patients with DIE compared to healthy women.
Methods
Full ethical approval of the study protocol was obtained from the local ethics committee. From September 2010 to April 2013, a consecutive series of 263 patients of the Minimally Invasive Gynaecological Surgery Unit, S. Orsola-Malpighi Hospital, University of Bologna, aged 18–40 years and with a diagnosis of DIE agreed to take part in the study protocol. Similarly, 250 healthy women were recruited from the hospital's family planning clinic.
All women with DIE underwent gynaecological examination and transvaginal and abdominal ultrasonography in order to evaluate the presence of pelvic endometriosis before surgery. Other diagnostic tests were performed when indicated as previously described.14 ,15 All women scheduled for laparoscopic management of DIE gave informed written consent to surgical treatment and to participate in this research anonymously. One day before surgery, patients were invited to complete the Italian translation of the Sexual Health Outcomes in Women Questionnaire (SHOW-Q).16 Women from our family planning clinic were asked to answer the same SHOW-Q questionnaire during routine evaluation.
Women with DIE underwent complete excision of macroscopic endometriotic lesions. Laparoscopic resection of endometriosis was performed as previously described.17–19 The surgical procedures were performed by the same surgeon (RS), and the surgical team had a consistent background in laparoscopic treatment of patients with DIE. After surgery, histological analysis was done and only after confirmation of the diagnosis were patients asked to continue with the postoperative phase of the study. Six months after surgery, patients underwent clinical examination and transvaginal ultrasonography to evaluate their symptoms and/or anatomical relapse of endometriotic nodules, and they were asked to complete the SHOW-Q questionnaire again. Postoperatively, all endometriosis patients received cyclical low-dose monophasic combined oral contraceptives, which have been shown to improve symptoms and sexual function.6 On entry to the study, participants were sexually active (having had sexual intercourse in the past 12 months and at least once in the past 3 months), with knowledge of the Italian language. Exclusion criteria were: previous or current gynaecological cancer, intestinal inflammatory disease, history of pelvic radiotherapy or systemic chemotherapy, history of gynaecological infection in the last 3 months, history of psychiatric disorder and use of psychotropic medications.
All women gave informed written consent to participate in the study and to the possible use of their anonymous data for research purposes. Participants were assessed regarding demographic and clinical characteristics [age, body mass index (BMI), parity and hormonal contraception]. They completed the anonymous SHOW-Q sexual function questionnaire in private.
The SHOW-Q questionnaire comprises 12 items organised conceptually to include two or three items per domain: satisfaction with sex, orgasm frequency, sexual desire, and pelvic problem interference with sexual functioning. Factor analysis had demonstrated that the 12-item scale had high internal consistency and reliability (Cronbach's α=0.86), with four reliable subscales (α=0.73 to 0.84).16 SHOW-Q is suitable for women of diverse socio-demographic and clinical backgrounds, including women in same-sex relationships and women who are sexually active without a partner. In addition, this questionnaire investigates different aspects of sexual life and interference with sexual functioning by pelvic problems. In responding to the questions, participants were asked to consider the previous 4 weeks. All sexual function item responses were converted to a scale of 0–100 points. Higher scores indicated better sexual functioning, except for pelvic problem interference in which a higher score indicated greater interference.
Statistical analysis
The Kolmogorov-Smirnov test showed that the clinical characteristics of the patients had a normal distribution (p>0.05). Therefore, to compare clinical characteristics between the study groups, Student's t-test was used. The comparison of SHOW-Q scores between ‘pre-surgery versus post-surgery’ and ‘post-surgery versus healthy women’ was performed using the Wilcoxon and Mann-Whitney U-tests, respectively, because the Kolmogorov-Smirnov test failed to show normal distribution (p<0.0001). For all tests p<0.05 was considered significant. Statistical analysis was performed using SPSS software V.15.0 (SPSS Inc., Chicago, IL, USA).
Results
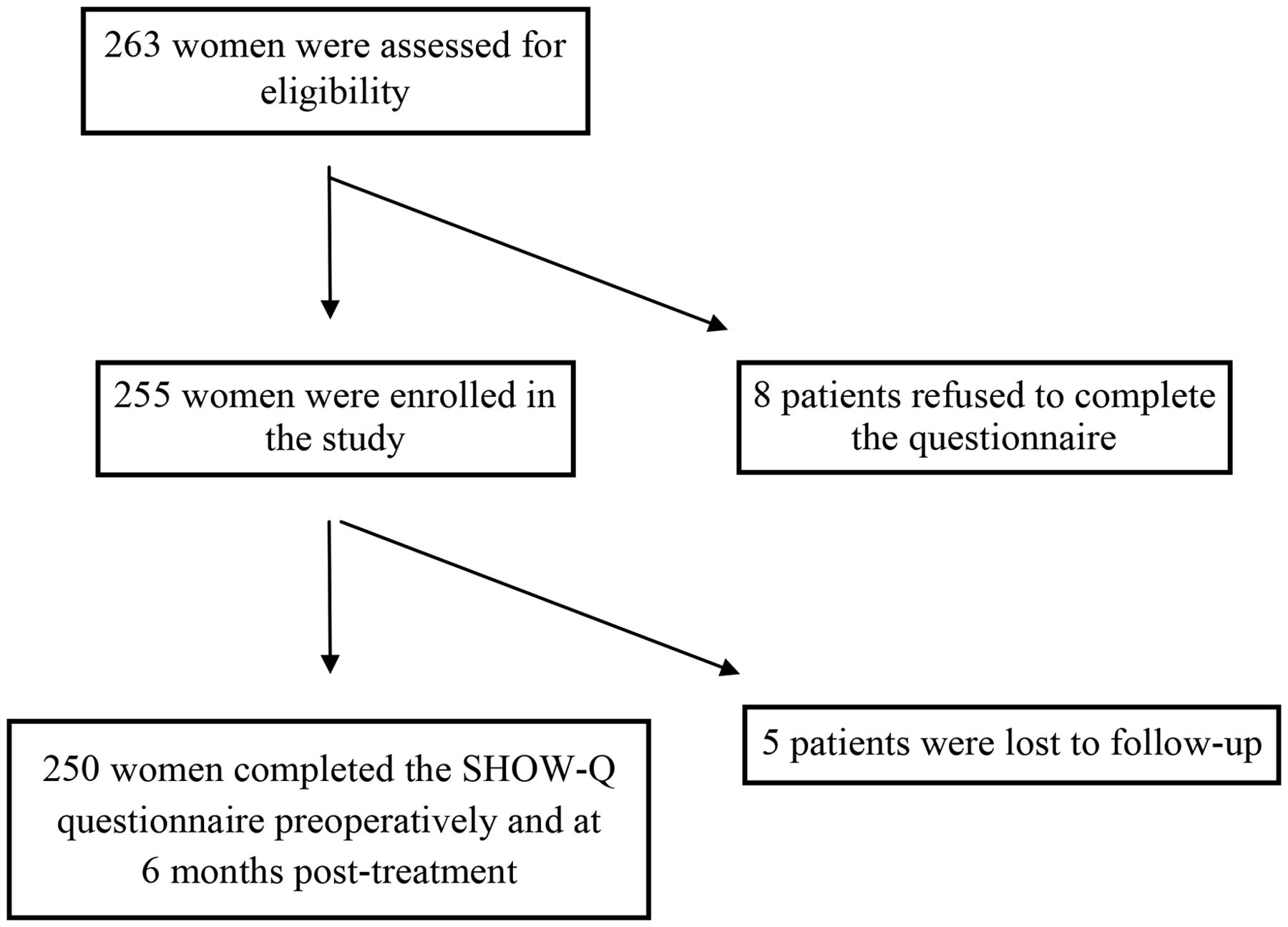
Of the 263 patients with endometriosis approached to participate in the study, 250 patients were finally included in the Endometriosis Group (Figure 1).
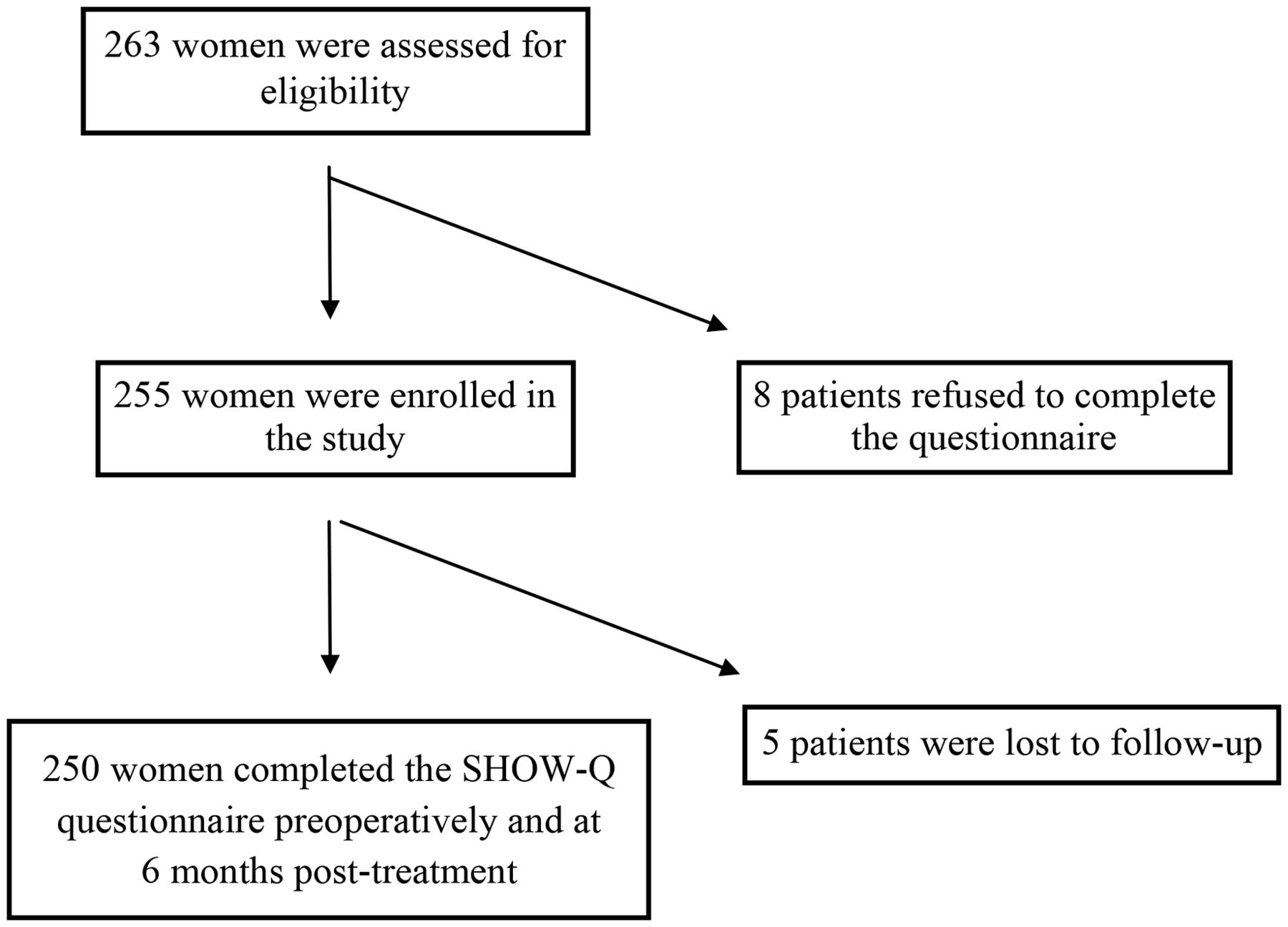
Study profile. SHOW-Q, Sexual Health Outcomes in Women Questionnaire.
Baseline demographic and clinical characteristics of all women involved in the study are described in Table 1. The two groups were homogeneous for all characteristics analysed (age, BMI and hormonal contraception) except for parity.
Demographic and clinical characteristics of the two study groups
We compared SHOW-Q scores in the endometriosis group before and 6 months after surgery with the healthy group (Table 2).
Sexual Health Outcomes in Women Questionnaire scores for patients with deep infiltrating endometriosis pre- and post-surgery and for healthy women
The distribution of post-surgery SHOW-Q scores was comparable to healthy women's scores apart from the orgasm scale score, which was unchanged in the post-surgery group.
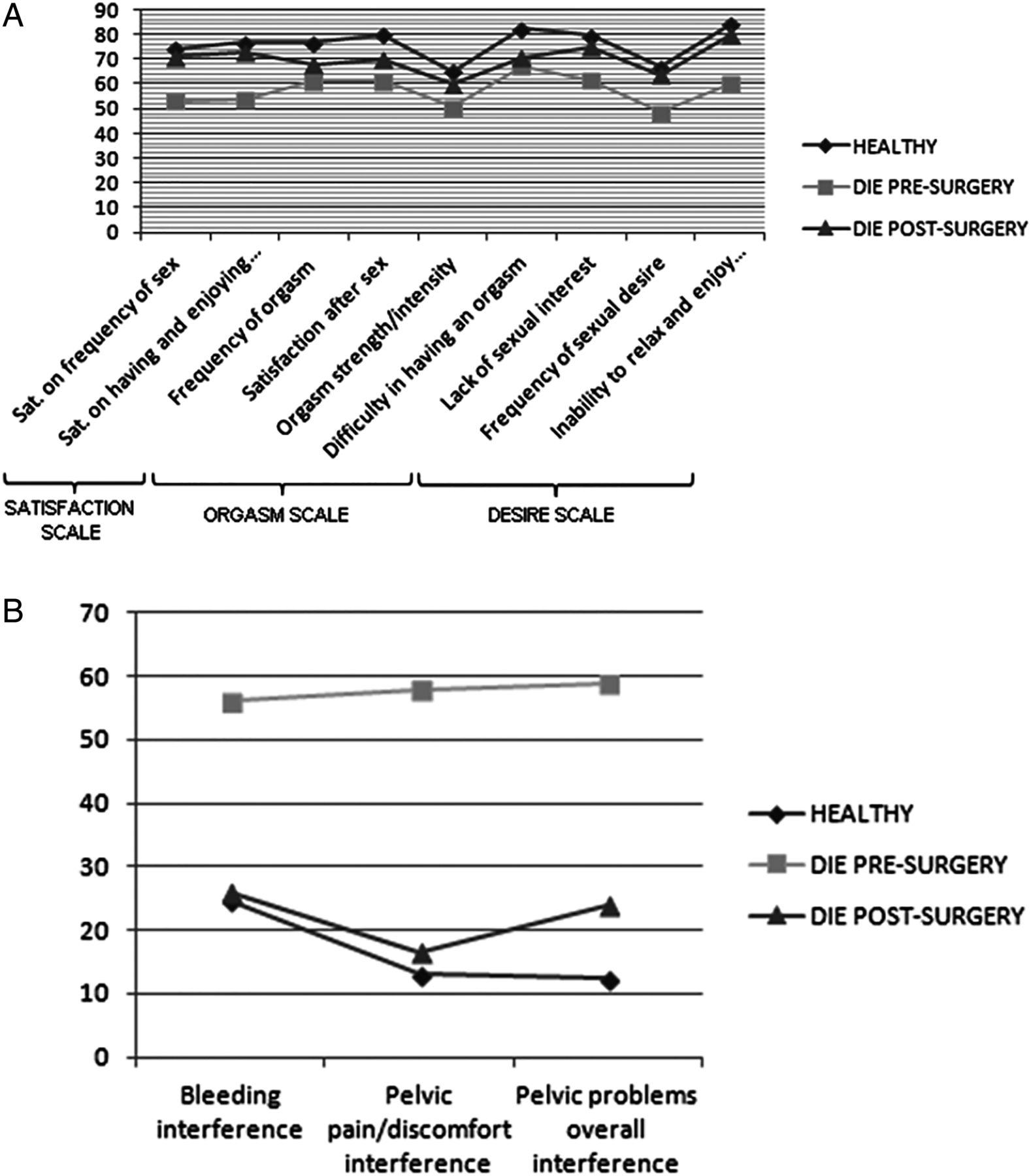
Significant increase in the satisfaction and desire scale scores was observed between pre- and post-treatment, and at 6 months follow-up patients treated for DIE showed no statistically significant differences in those scores compared to healthy women (Figure 2A).

{kind=link}
{kind=link}
Sexual Health Outcomes in Women Questionnaire (SHOW-Q) profile of question-specific scores in patients with deep infiltrating endometriosis (n=250) before and at 6 months post-treatment, compared with 250 healthy women. (A) Satisfaction, orgasm and desire scales. (B) Pelvic problem interference scale. DIE, deep infiltrating endometriosis; Sat, satisfaction.
Regarding the orgasm scale, we did not find any improvement comparing pre- and post-treatment. Moreover, the orgasm scale score was statistically significantly higher in healthy women than in DIE patients either before or after surgery (p<0.001).
Concerning the pelvic problem interference scale, a significant improvement was found comparing pre- and post-treatment (p<0.001). At 6 months after surgery, results were similar to healthy women with no statistically significant differences between the two groups (Figure 2B).
Discussion
In this study, we hypothesised that surgical management of women with DIE might have a positive impact on the SHOW-Q score, indicating an improvement in overall sexual function. We sought to compare sexual function between patients affected by DIE and healthy women.
Sexual function involves a wide and complex range of local organic, neurological, psychological and environmental factors that affect not only physical but mental health, as well as feelings of femininity and relationships.20–22 Furthermore, infertility and depression, which are highly prevalent in women with endometriosis, are also associated with the impairment of sexual function.23 ,24 Recently medical interest in sexual function in women with endometriosis has increased.
In our previous study, sexual function in patients with DIE and in healthy women was reported.25 We found that every area of sexual function investigated through the SHOW-Q questionnaire (satisfaction, desire, orgasm and pelvic problem interference) was significantly impaired compared to healthy women.25 Moreover, several studies have demonstrated that surgical excision of deep endometriotic lesions markedly reduces the severity of dyspareunia and improves the quality of sexual function in these patients.22 ,26 ,27 Women affected by endometriosis, especially DIE, benefit from the combination of laparoscopic surgery and postoperative hormonal therapy, which has been shown to improve symptoms and sexual function.6 ,20 ,22 ,28 ,29 In line with this, our results have demonstrated that in patients treated for DIE, sexual function was generally comparable to healthy women 6 months postoperatively.
Different types of questionnaire have been used in the last few years to investigate sexual function in women with endometriosis.4 ,6 ,29–32 We chose the SHOW-Q questionnaire for its brevity, evidence of validity and reliable subscales (satisfaction with sex, orgasm frequency, sexual desire and pelvic problem interference with sex).16
In particular, we found a significant improvement post-treatment in the areas of satisfaction, desire and pelvic problem interference, and no differences between patients treated for DIE and healthy women. Sexual desire and satisfaction are profoundly influenced by emotion and they are governed by a complex of inhibitory and excitatory influences. Women with dyspareunia often develop Hypoactive Sexual Desire Disorder (HSDD) or arousal disorder because pain is both a potent inhibitor of the sexual response cycle and a potent modifier of behaviour.33 Probably women treated for DIE, after surgery, managed to relax and feel more comfortable during intercourse because of the reduction of pain symptoms and the awareness of the removal of endometriotic lesions. In a previous study we showed that the number of DIE nodules was directly proportional to reduction of sexual desire.4 Advanced stages of disease may affect several aspects of women's lives including psychological areas. It seems therefore that mental and physical health may impact deeply on these spheres of sexual function.33
Moreover, DIE is strongly associated with chronic pelvic pain. Around 40% of women with endometriosis and chronic pelvic pain have sexual dysfunction and decreased frequency of sexual intercourse.31 Pain during intercourse has been associated with the involvement by DIE of the uterosacral ligaments, pouch of Douglas, posterior vaginal fornix and anterior rectal wall.32 ,34–37 In line with our findings, a recent study showed that the most positive effect of surgery was seen in painful sexual intercourse.38 This result could be explained by the fact that the complete excision of all endometriotic lesions and the restoration of normal pelvic anatomy might reduce interference with sex by pelvic problems.
However we could not limit the sexual function evaluation to the presence or not of pelvic pain,20 since its alleviation, as we demonstrated, did not improve all areas of sexual function. Specifically, we observed that the laparoscopic management of DIE did not significantly improve the orgasm scale. It is difficult to explain this result, since orgasm is a complex phenomenon that has a multifactorial genesis, depending on psychological, anatomical and physiological factors.32 Regarding anatomical factors, it is known that radical surgery for endometriosis carries a potential risk of autonomic nerve damage and consequent impairment of orgasm.
We are aware that this study has a number of limitations that should be taken into account when interpreting the results. First, all women affected by DIE used hormonal therapy before and after surgical treatment, since leaving them without any medical therapy for the purpose of the study was unethical given its importance in preventing disease and symptom recurrence. It is important to underline that the specific effects of hormonal contraception on female sexuality are not yet well understood, since female libido is complex and it is difficult to reliably predict how it might be affected by hormonal therapy.39 Current literature suggests that there are mixed effects on libido, with a small percentage of women experiencing an increase or a decrease, and the majority being unaffected.39
Second, the study was conducted in a tertiary care centre for endometriosis treatment where most of the patients had a severe stage of the disease; therefore participants in the study might not be representative of the entire population affected by endometriosis. Obviously, impairment of sexual function in patients with advanced stage disease is likely to be greater compared to patients with less severe disease.
Third, although women answered the SHOW-Q questionnaire anonymously, alone and in a private room, there is a high risk of both response and recall bias due the questionnaire's enquiry about aspects of sexual function that many women consider to be of a very private nature. Studies of human sexuality are prone to bias and have confounding factors because of the wider cultural context as well as psychosocial factors that define this aspect of human behaviour.
This study does, however, have a number of strengths. First, healthy women were recruited from the family planning clinic and had no benign gynaecological disorders such as myomas, polyps or polycystic ovary syndrome. Second, the study is original in evaluating sexual function in women affected by DIE both before and after surgery compared to healthy women. Third, the study had a large number of participants. Finally, all patients who underwent surgery had a histologically confirmed diagnosis of DIE.
In conclusion, we found that after surgery, sexual function of women affected by DIE was generally comparable to that of healthy women. Satisfaction, desire and pelvic problem interference scales were significantly improved after surgical treatment. The surgical approach could have a positive impact not only on organ impairment but also on sexual function in women affected by DIE, and female sexual health concerns should therefore be integrated into routine gynaecological care.
References
Footnotes
Competing interests None.
Ethics approval The study received ethics approval from the institutional ethics committee responsible for human experimentation (Comitato Etico Indipendente dell'Azienda Ospedaliero-Universitaria di Bologna, Policlinico Sant'Orsola-Malpighi) [Date of approval: 16 December 2008; Reference number: 155/2008U/Oss].
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue