Article Text

Abstract
Objectives In an attempt to understand the demand and main drivers of telemedicine abortion, we analysed the requests that Women on Web (WoW), an online telemedicine abortion service operating worldwide, received from France throughout 2020.
Methods We conducted a parallel, convergent, mixed-methods study among 809 consultations received from France at WoW between 1 January and 31 December 2020. We performed a cross-sectional study of data obtained from the WoW consultation survey and a manifest content analysis of anonymised email correspondence of 140 women consulting with the WoW helpdesk from France.
Findings We found that women encounter macro-level, individual-level and provider-level constraints while trying to access abortion in France. The preferences and needs over secrecy (n=356, 46.2%), privacy (n=295, 38.3%) and comfort (n=269, 34.9%) are among the most frequent reasons for women from France to choose telemedicine abortion through WoW. The COVID-19 pandemic seems to be an important driver for resorting to telemedicine (n=236, 30.6%). The lockdowns had a significant impact on the number of consultations received at WoW from France, increasing from 60 in March to 128 in April during the first lockdown and from 54 in October to 80 in November during the second lockdown.
Conclusions The demand for at-home medical abortion via teleconsultation increased in France during the lockdowns. However, drivers of telemedicine abortion are multidimensional and go beyond the conditions unique to the pandemic.
- abortion
- induced
- health services accessibility
- reproductive medicine
Data availability statement
All original data are available upon reasonable request to the researchers.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Key messages
Women continue to encounter macro-level, individual-level and provider-level constraints in accessing abortion care in France.
The demand for telemedicine abortion received at Women on Web from France has increased significantly during lockdowns; from 60 in March to 128 in April during the first lockdown and from 54 in October to 80 in November during the second lockdown.
The preferences and needs over secrecy (n=356, 46.2%), privacy (n=295, 38.3%) and comfort (n=269, 34.9%) are among the most frequent reasons for women from France to choose telemedicine abortion through Women on Web.
Introduction
The COVID-19 outbreak has posed significant challenges for the provision of abortion care. In the context of the pandemic, national abortion guidelines in France have changed several times. In April 2020, France introduced a temporary exemption from the requirement to take the abortion medication in the presence of a medical doctor or midwife and allowed at-home medical abortion via teleconsultation until 7 weeks of gestation (9 weeks of amenorrhoea).1 The measure was adopted in the midst of a national lockdown, which started on 17 March 2020 and continued until 11 May 2020, and was justified as per the recommendations of the World Health Organization (WHO), advances in telemedicine, and the “strong mobilisation of the health establishment in the management of the crisis and the need to limit consultations in hospitals for any other reason”.1 2 The measure allowed women to book appointments online, purchase abortion pills from a pharmacy on prescription, and self-manage their abortions at home. Abandoned in July, the same measure was once again embraced in November as the health crisis intensified.3 It was affirmed that medical abortion pills can be delivered directly to individuals in pharmacies with an ‘exceptional delivery’ (délivrance exceptionnelle) notation. Similar to the previous measure, this decree was also adopted in the middle of a second nationwide lockdown, which started on 30 October and continued until 15 December 2020.
The French abortion guidelines allow abortions to be performed until 12 weeks of gestation (14 weeks of amenorrhoea).4 Ultrasound prior to abortion is not required.5 Since 2016, midwives are authorised to practise medical abortions and every procedure required within the framework of abortion care, including ultrasound and post-abortion care, is fully reimbursed by social security for all women, including undocumented immigrants.6 7 Before the COVID-19 pandemic, telemedicine abortion provision was not allowed; individuals were instead required to take the first abortion medication, mifepristone, in the presence of a medical doctor or a midwife.4 Medical abortions until 5 weeks of gestation (7 weeks amenorrhoea) were performed in private offices of doctors and midwives, primary care centres (centre de santé), family planning centres or in hospitals. Between 5-7 weeks gestation (7-9 weeks of amenorrhoea), medical abortion was performed only in clinical settings; women were required to take the first abortion medication, mifepristone, in a clinic or hospital and had to return 48 hours later to take the second medication, misoprostol. They were then required to stay at the clinic or hospital for at least 3 hours following misoprostol administration.4
France was not the only country in Europe to reconsider the regulations governing the dispensation of medical abortion pills during the pandemic. Similar measures were also adopted in England, Wales, Scotland and Ireland.8 These measures were often based on recommendations and guidelines of the WHO, recommending telemedicine and self-care interventions for the provision of medical abortion within the first trimester (12 weeks of gestation).9 In fact, rights groups and experts have previously challenged the ‘overregulation’ of abortion pills10 and have been calling for abortion pills to be available in pharmacies11 and for home medical abortion to be provided via telemedicine prior to the pandemic.12 Given that certain countries facilitated expanded access to abortion pills with the COVID-19 outbreak, several groups and practitioners now call for the adopted measures to continue beyond the pandemic.13 14
In the light of these recent changes and debates, we examined why women chose at-home abortion via teleconsultation in France. With this objective, we analysed help requests that Women on Web (WoW), an online telemedicine abortion service operating worldwide, received from France throughout 2020. WoW only works in countries with restrictive abortion laws and previously did not accept consultations coming from countries where abortion is legal and accessible; the WoW website rather directed women from these countries to local services. However, the organisation enabled consultations from some countries where abortion is legal for research purposes. Within this framework, WoW enabled its online consultation for individuals from France starting from 1 January 2020. Our research analyses consultations WoW received from France to provide insights into women’s motivations for resorting to telemedicine abortion.
Methods
We conducted a parallel, convergent, mixed-methods study among the 809 consultations received from France at WoW between 1 January and 31 December 2020. Within the framework of this research we had two main data components. The first component was quantitative data obtained from WoW consultation questionnaires and the second was qualitative data obtained from women’s anonymised email correspondence with the WoW helpdesk. Both components were collected simultaneously and analysed independently. Participants agreed to their anonymous data being used for research purposes.15
Quantitative analysis
We performed a cross-sectional study of the survey data obtained from the WoW consultation survey that participants completed while requesting help online. The WoW consultation process has been described previously.16 The WoW consultation survey consists of 25 questions and is available online on the WoW homepage.17 The survey consists of both categorical and continuous data. It includes demographic questions about age and country, medical questions about pregnancy (gestation), contraceptive behaviour, previous pregnancy and abortion experience, and medical contraindications, and research questions about reasons for wanting an abortion and choosing telemedicine through WoW. Within the framework of this study, we analysed responses on age, pregnancy, including gestation, previous pregnancy and abortion experience, contraceptive behaviour, and reasons for wanting an abortion and choosing telemedicine through WoW. We summarised continuous data as medians and interquartile ranges, and categorical data as frequencies. The data analysis was done using IBM SPSS Statistics for Macintosh, Version 27.0 (IBM Corp., 2020).
Qualitative analysis
When women from France completed their online WoW consultations, they were given information on local abortion services and were asked:
If you are unable to access abortion services in France, could you please tell us a bit more about why? […] We will let you know as soon as possible if we can help you in any way.
In order to better understand women’s motivations for choosing telemedicine, and also to map the perceived barriers of access to abortion in France, we conducted a manifest content analysis of women’s anonymised email correspondence. Not all women who filled in the online consultation at WoW website proceeded with email correspondence. Two researchers (HA and EL) analysed the email correspondence of those who did until data saturation was reached, when new data started to be redundant in relation to the data already collected. In total, 157 emails were analysed at the manifest level from correspondence with 140 women. Emails varied in length from 4 to 540 words. The content analysis was conducted in NVivo (QSR International Pty Ltd, March 2020). All researchers contributed to the identification and categorisation of the emergent themes, and the themes were quantified for the analysis.
Findings
Quantitative findings
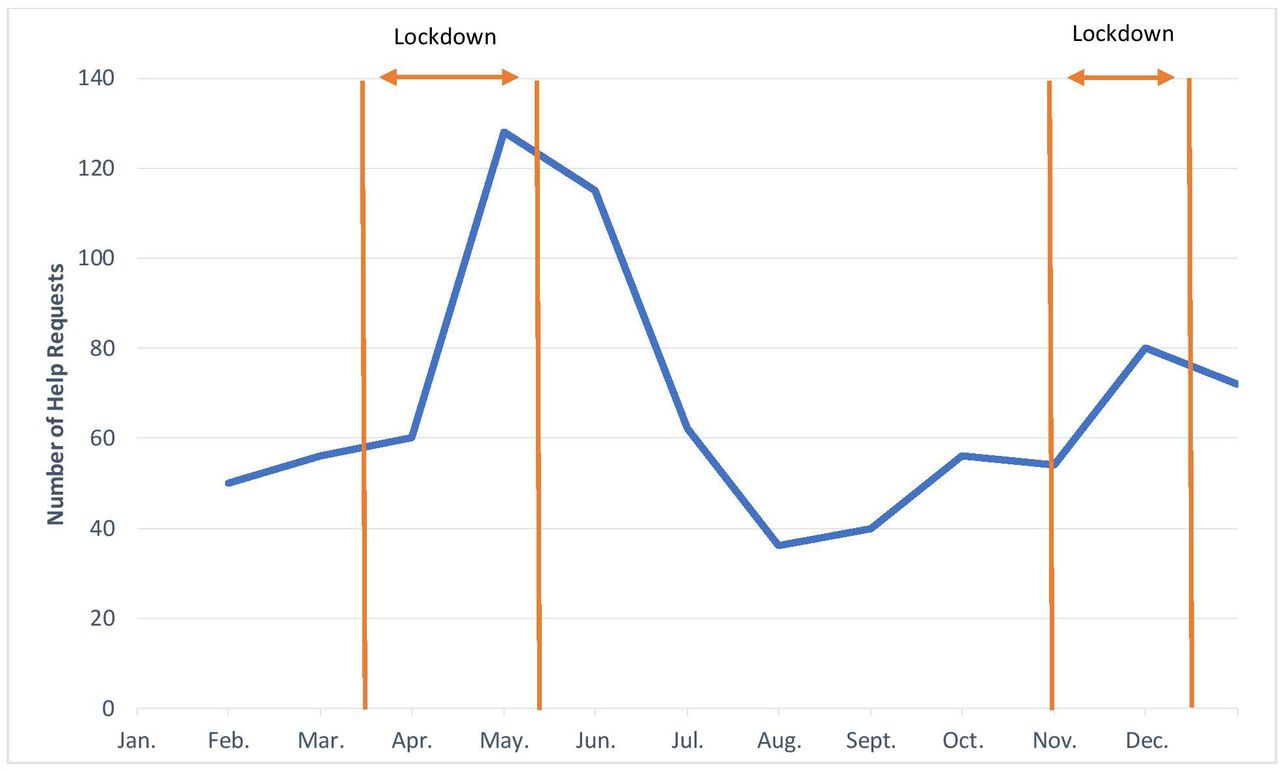
Between 1 January and 31 December 2020, 809 women from France completed an online consultation on the WoW website in which they requested telemedicine abortion services. This time period also coincided with a highly challenging health emergency: the COVID-19 pandemic. The health emergency and associated lockdown measures restricted mobility, thereby adversely affecting availability of services including abortion care. Throughout 2020, the French government took several measures to reduce the spread and transmissions of the coronavirus, including nationwide lockdowns (confinement national) – the first from 17 March to 11 May and the second from 30 October to 15 December 2020. Lockdowns entailed closure of borders, schools and offices, and strict travel restrictions, all reinforced by the penalisation of offences related to the emergency measures. It is in this context that figure 1 illustrates the number of telemedicine abortion consultations received from France at WoW during 2020; the consultations significantly increased during the lockdowns; from 60 in March to 128 in April during the first lockdown and from 54 in October to 80 in November during the second lockdown.
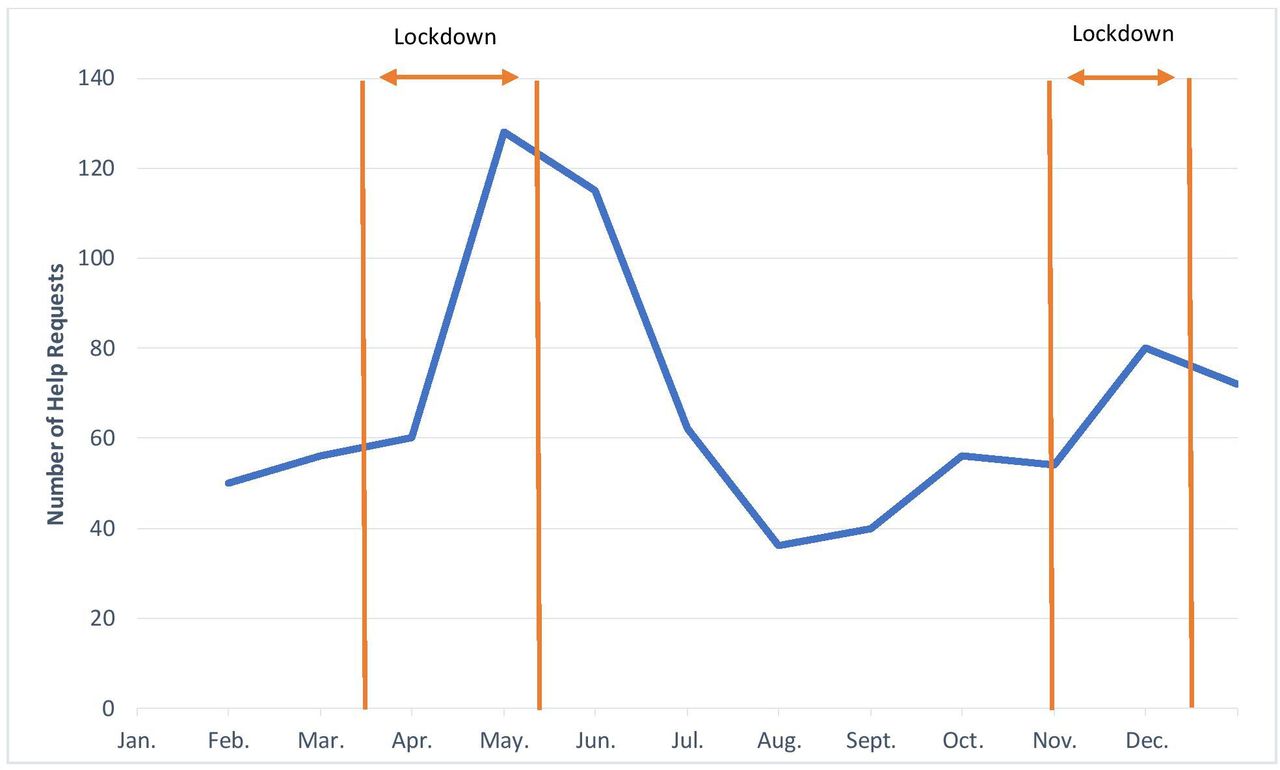
Number of telemedical abortion consultations from France received by Women on Web between 1 January and 31 December 2020 (n=809).
Table 1 summarises the background and pregnancy- and abortion-related experiences of women. Table 2 illustrates the reasons why women from France requested telemedicine abortion through WoW. We differentiated women's reasons according to age in order to map demographic patterns. We also distinguished between consultations where COVID-19 was mentioned and not mentioned among reasons given, to suggest a counterfactual effect for reasons within and outside the pandemic context.
Background and pregnancy- and abortion-related experiences of women from France requesting telemedicine abortion through Women on Web between 1 January and 31 December 2020
Reasons why women chose telemedicine through Women on Web between 1 January and 31 December 2020 according to age group and COVID-19 relevancy
While the lockdown measures increased the demand for telemedicine abortion in France, the drivers of telemedicine are manifold. The preferences and needs over secrecy (46.2%), privacy (38.3 %) and comfort (34.9%), followed by coronavirus pandemic (30.6%), were among the most frequent reasons for women to choose telemedicine abortion in France. Women also indicated a preference to take care of their own abortions as their reason for choosing telemedicine through WoW, demonstrating a salient willingness to self-manage their abortion (28.6%). We found that similar frequencies, with slight fluctuations, are observed among COVID-19-related and -unrelated consultations with the exception of willingness for self-management, which appears to be exclusive to COVID-19-unrelated consultations. We noted that compared with women aged over 36 years, younger women aged 18–25 years are twice as likely to find at-home abortion via telemedicine empowering and three times more likely to prefer having someone with them during the procedure compared with women aged over 36 years. They are, however, also twice as likely to perceive abortion stigma and 53.5% more likely to need to keep their abortion secret from their family or partner. Finally, younger people are also twice as likely to encounter financial difficulties while accessing abortion care in France.
Qualitative findings
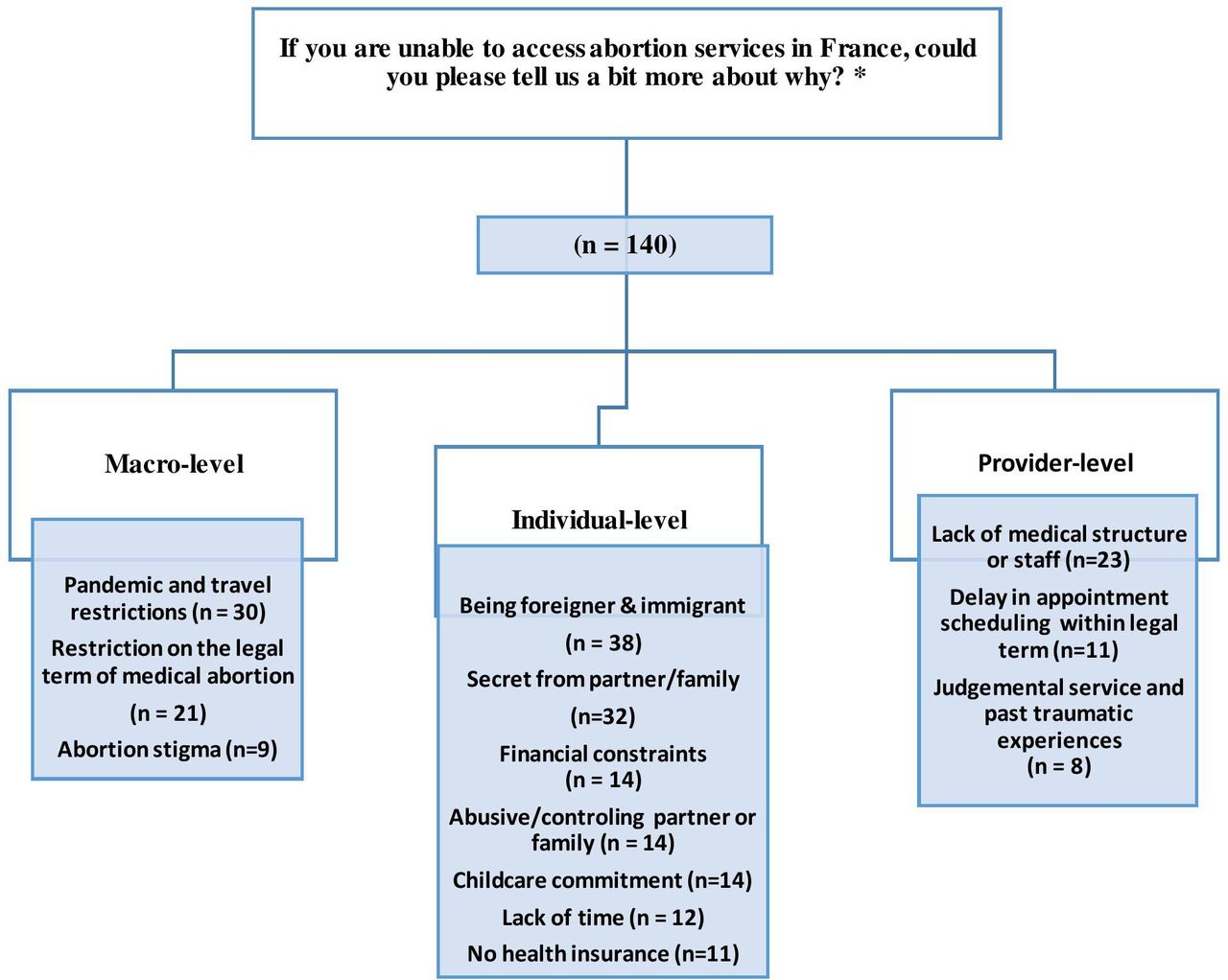
In figure 2, we grouped women’s replies in three main categories: macro-level constraints, individual-level constraints and provider-level constraints. Macro-level constraints include sociopolitical conditions and legal frameworks, individual-level constraints concern women’s personal circumstances and preferences and, lastly, provider-level constraints entail issues raised around service provision and access to available care.

{kind=link}
{kind=link}
Schematic presentation of categories and subcategories derived from the email correspondence of 140 women from France who consulted Women on Web between 1 January and 31 December 2020. *Women often had multiple constraints that cut across different categories and subcategories, and therefore the sum of correspondents for all categories exceeds the overall number of respondents.
In their email correspondence, women reported not being able to access abortion care in France due to the pandemic and travel restrictions. As existing health structures were overburdened by the ongoing health emergency, women wrote about not being able to find or travel to an available medical facility or practitioner for abortion. A young woman’s email epitomises this situation:
I can’t get an abortion as my family doesn’t know that I’m pregnant, and if they do find out, I’m in big trouble. I live in a village and it is actually not possible for me to access abortion unless I travel to Switzerland, which is not an option now due to lockdown. The closest clinic is 2 hours away and I cannot travel that far.
Delays in scheduling appointments, combined with the restriction on the legal term for medical abortion, appeared to be a frequent concern among many women consulting WoW. Several emails involve women contacting local clinics and associations and not being able to schedule an appointment within the legal gestational limit for medical abortion. A woman who was in such a situation wrote:
I want to remain in the legal time limit for medical abortion, but I could not find any place to go before 2 months. I will pass the legal limit by then!
We observed that most of the time, women experience multiple constraints at the same time, which later informs their preferences. One woman requesting service wrote:
I’m writing to you after being refused by three gynaecologists, they all refer me to the hospital which is overburdened with COVID-19. I contacted the family planning clinic, one is closed today, the other does not want to take me because I am not from their city. Besides the family planning clinic is difficult, they ask for two appointments, 1 day of hospitalisation and a check-up. I have two jobs to get by financially. I have experienced an abortion this way before, it was traumatic. I’d rather be at home and manage my own abortion.
Even when abortion care is available and supposedly accessible, women reported personal circumstances that prevented them from accessing abortion care. These circumstances entailed being immigrant, wanting to keep the abortion secret, experiencing financial constraints, violence, abuse, or living in a controlling environment. Childcare commitments, lack of time due to work or school, and not having health insurance were also mentioned among obstacles women encounter in accessing local care. One woman who experiences violence wrote:
I know abortion is legal in France, but I will tell you why I will not be able to have an abortion here. My companion is a violent man, I will never be able to have the opportunity to go to a hospital or a centre, without him watching me.
Another email reflects the difficulties of a young foreign student who has no access to French national healthcare due to financial difficulties and lack of insurance coverage:
I called to make an appointment with the public hospital, and I was notified that the cost for an abortion is 630 Euros, of which I am totally not within the financial means to handle. I am a foreign student in France and because of the complications due to COVID-19, I’m currently in the process of renewing my student visa. However, my current visa is expired. Because of this as well, I don’t have access to the French national healthcare and unfortunately I am not insured in France. My parents who are my main financial support are very conservative and would not support paying that much for the abortion.
Women also mentioned encountering stigma and judgement. Some women had past traumatic experiences and hence indicated their preference for telemedicine abortion at home. A woman who fears judgement and pressure from medical staff wrote:
Working in a hospital myself and having had abortion 2 years ago, I am really afraid of being judged. In my region, getting an abortion is an obstacle course. The city gynaecologist does not perform abortions and doctors here rather pressure you to continue with pregnancy.
Discussion
The drivers of telemedicine are multidimensional and go beyond conditions unique to the pandemic. Rather than creating new challenges, the COVID-19 pandemic has in fact illuminated and further amplified precipitating malfunctions in abortion care provision.18 Previous research on abortion access in France has demonstrated an unequal recourse rate across French territories varying from 11.8 per 1000 women in Pays de la Loire in metropolitan France to 39 per 1000 women in overseas territories like Guadeloupe and Guyana.19 Moreover, the question of gestational limit for abortion has been frequently problematised within the French context. It is estimated that each year 3000–5000 women travel abroad to have an abortion, notably to Spain and to the Netherlands, because they have passed the permitted gestational limit in France.20 Recourse to and drivers of induced abortion, as well as women’s experiences with local abortion care or travelling abroad to seek care, have been extensively studied within the French context.21 22 Expanding on this literature, this article provides initial insights into the drivers of telemedicine abortion in France by analysing women’s motivations and perceived barriers of access to abortion care.
Our study shows that while the coronavirus and related pandemic restrictions constituted an important push factor for women to choose telemedicine, the drivers of telemedicine are manifold and not unique to the conditions related to the pandemic. Our research findings suggest that telemedicine can help meet women’s needs and preferences for secrecy, privacy and comfort, while facilitating increased access and enabling more person-centred abortion care. Given the inequality of access, together with the macro-, individual- and provider-level challenges women face as regards accessing abortion care, telemedicine can also help extend access to abortion in places where it remains limited, including rural areas. Improving access and adopting a person-centred approach to abortion care are likely to benefit those who are most vulnerable, living under resource-poor or financially dependent circumstances, and grappling with higher rates of stigma and judgement.23
The WHO contends that at-home abortion via teleconsultation is acceptable, non-invasive and cost effective.9 It further suggests that self-management of abortion at home improves autonomy, by enabling a sense of control over one’s own body and the abortion procedure.9 In the context of the pandemic, several studies attest to increased demand for abortion via teleconsultation. Aiken et al, for instance, found that the rate of requests for at-home medical abortion across the United States increased by 27% from March to April in 2020.24 Research conducted with WoW data on consultations received from eight European countries between 1 January 2019 and 1 June 2020 also found a significant increase among the consultations received from Hungary, Italy, Malta, Northern Ireland and Portugal.25 No increase was observed in the number of consultations from Great Britain, Germany and the Netherlands.25 Our research also contributes to these studies by demonstrating trends from France throughout the pandemic in general and during lockdowns in particular. Moreover, our research findings provide the grounds for comparison of the drivers of telemedicine in France with those in different countries. We found it important to note, for example, that compared with previous research conducted with WoW data on Germany in 2019, cost and stigma are each much less of a driver in France (respectively 20.2% and 11%) than in Germany (respectively 40.2% and 37.4%).26
Endorsed by the WHO, telemedicine came to the fore as the silver lining amid the COVID-19 pandemic.27 Examining some immediate impacts of telemedicine abortion provision in the UK, a recent study found that introduction of telemedicine for abortion care during the pandemic has reduced the waiting times for termination by 4.2 days and also that more abortions were provided at less than 6 weeks’ gestation with telemedicine.28 Another study examining at-home abortion by telemedicine at less than 12 weeks’ gestation in Scotland during the pandemic suggests that abortion without routine ultrasound is safe, and has high efficacy and high acceptability among women.29 Further research should examine the impact of telemedicine abortion provision on the French health system to better inform COVID-19 response and policymaking during and beyond the pandemic.
Study strengths and limitations
The WoW dataset consists of self-reported data, which is one of the major limitations of this study. The cross-sectional data are derived from a defined list of motivations and reasons, asking survey respondents to check the options which correspond to their situation. Multiple answers were allowed. The participants’ responses herein might involve acquiescence bias. The data for France were collected only for 2020, and therefore we could not conduct a multi-year longitudinal analysis to gauge the impact of the pandemic on the overall demand for telemedicine abortion. The content analysis could have been enriched with in-depth qualitative interviews.
Despite these limitations, the study offers a significant contribution to the literature on abortion access in France during the pandemic. To our knowledge, there is no study on the demand for and drivers of telemedicine abortion in France. Given the ongoing health emergency, the study has significant potential to inform policymakers on telemedicine abortion care provision within the French context but also in other similar contexts. Previous research conducted with the same dataset for other countries also provides us with the opportunity to compare the French situation with that in other countries.30
Abstract translation
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.Data availability statement
All original data are available upon reasonable request to the researchers.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the Regional Ethics Committee, Karolinska Institutet, Dnr 2009/2072-31/2 and Dnr 2020/05406.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @hazalatay7
Contributors HA conceived the original research question. HA and EL performed both the quantitative analysis and the qualitative analysis. HP and KGD supervised the study analysis. HA wrote the article manuscript. All authors participated in the discussion of the results and approved the final version of the manuscript.
Funding This research was funded by a public grant overseen by the French National Research Agency (ANR) as part of the “Investissements d’Avenir” programme LIEPP (ANR-11-LABX-0091, ANR-11-IDEX-0005-02) and the Université de Paris IdEx (ANR-18-IDEX-0001).
Competing interests Coauthors RG and HA work for or are affiliated with Women on Web.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.