Article Text

Abstract
Background Hormonal contraceptives are the most common method used worldwide by teenagers to prevent unwanted pregnancies. To date there are limited data about such use by teenagers in the UK. This study investigated trends and patterns of hormonal contraceptive prescribing to adolescents aged 12–18 years in UK primary care between 2002 and 2011.
Methods A retrospective cohort study using the IMS Disease Analyzer database was conducted. All females aged 12–18 years with ≥1 prescription for a contraceptive drug between 1 January 2002 and 31 December 2011 were included. Annual prevalence of contraceptive drug prescribing was calculated, and indications for prescribing, and types of contraceptive drug prescribed, were examined.
Results In 2002, 13.7% (6135/44 532) of female adolescents received prescriptions for hormonal contraceptives, compared to 19.0% (6597/34 676) in 2011. The majority of female adolescents [2002: 76.2% (4676/6135); 2011: 65.7% (4334/6597)] received a contraceptive drug for ‘contraceptive management’. The combined oral contraceptive (COC), ‘progestogen+estrogen’, was the most commonly prescribed. Although use of progestogen-only contraceptives was lower than COCs, the number of patients who received desogestrel pills and etonogestrel implants increased during the study period; levonorgestrel pill use declined. Only one injectable progestogen, long-acting depot medroxyprogesterone acetate, was prescribed.
Conclusions Use of hormonal contraceptives among adolescents increased between 2002 and 2011, and COC usage was dominant. The increasing use of hormonal contraceptives in adolescents, especially in younger adolescents, warrants further investigation, including research into the long-term safety of these medicines in this age group.
- hormonal contraception
- teenagers
- family planning service provision
- genitourinary medicine
- oral contraceptives
Statistics from Altmetric.com
- hormonal contraception
- teenagers
- family planning service provision
- genitourinary medicine
- oral contraceptives
Key message points
The use of hormonal contraceptives by female adolescents in the UK increased during the study period, 2002 to 2011.
The contraceptive method most commonly prescribed to the study cohort was combined oral contraceptives.
Research into the safety of long-term use of hormonal contraceptives by adolescents is needed.
Introduction
Adolescents are an age group at high risk of unintended pregnancy and the importance of safe sexual activity among adolescents has been recognised worldwide.1 ,2 In 2001, a report by United Nations Children's Fund (UNICEF) showed that in 1998 the UK had the highest teenage birth rate (30.8 per 1000 women aged 15–19 years) in Western Europe.2 The UK government therefore launched a 10-year national Teenage Pregnancy Strategy in 1999.3 This national strategy aimed to halve the conception rate in those aged under 18 years by 2010 and establish a firm downward trend in those aged under 16 years, increase the proportion of teenage parents in education, training or employment to 60% by 2010, and reduce their risk of long-term social exclusion.3 Following the launch of this strategy the conception rate for those aged under 18 years decreased by 34% between 1998 and 2011.4
A study from the USA demonstrated an approximately 23% decline in birth rate for teenagers aged 15–19 years between 1995 and 2002.5 The authors stated that the decline of teenage pregnancy may be attributed to the improvement of contraceptive use in the USA.5 Though injectable hormonal contraceptives [e.g. depot medroxyprogesterone acetate injection (DMPA)] were considered among the most effective contraceptives, oral hormonal contraceptives were preferred by most female adolescents due to their effectiveness and ease of use.6 ,7
Patterns in the prescribing of combined hormonal contraceptives have changed over time (e.g. with the introduction of newer progestogens)8 but there is controversy regarding the risk of venous thromboembolism (VTE) with the different generations of combined pills.9–13 In January 2013, the Pharmacovigilance Assessment Committee (PRAC) at the European Medicine Agency (EMA) was asked by France to review the safety of the third- and fourth-generation combined oral hormonal contraceptives (COCs) due to concerns of a higher risk of VTE with these pills compared to first- and second-generation pills.14 The PRAC completed its report in October 2013 and concluded that the benefits of all combined hormonal contraceptives in preventing unwanted pregnancy outweigh their risk of VTE.15
A study conducted in UK, using the General Practice Research Database (GPRD) to investigate the level of combined contraceptive pills prescribed to women aged less than 16 years in general practice in 1997,16 showed that only 4.2% of teenagers aged 13–15 years received combined pills that year. The authors stated that the usage of the combined pill was low, considering that an estimated one-third of women aged less than 16 years were sexually active. They also stated that the low level of use of the combined pill may partially explain the high teenage birth rate in the UK compared to Western Europe.16 However, this study only investigated combined contraceptive pill use in 1 year, so it did not demonstrate the trends of contraceptive drug prescribing in female adolescents.
Despite the reduction of teenage pregnancy rates following the introduction of the UK government's Strategy on Teenage Pregnancy,3 the UK still has the highest rate of teenage pregnancy in Western Europe and so further reduction is needed for it to be on a comparable level with that of other Western European countries.17 Oral contraceptives are the most common contraception method used by female teenagers, so information about prescribing practices is necessary to prioritise further research into the use and long-term safety of hormonal contraceptive in this particular patient population. Hence, a cohort study based on a primary care health records database was conducted to investigate the current prescribing patterns of systemic hormonal contraceptives among a cohort of female teenagers aged 12–18 years between 2002 and 2011.
Methods
Study design
A descriptive cohort study was conducted using the IMS Disease Analyzer (IMS DA) to investigate the prescribing trends and patterns of hormonal contraceptives, indications for prescribing and the type of hormonal contraceptives drug used in female adolescents in UK primary care.
Data source
IMS DA contains anonymised computerised information systematically recorded by UK general practitioners (GPs). This database contains drug prescriptions, diagnoses and demographic data directly obtained from GPs’ computers. The data are derived from electronic health records in the GP practices via standardised interfaces and provide daily routine information on patients’ diseases and therapies. A practice transmits patient data stored in their GPs' computers to IMS DA on a monthly basis, after the data are encrypted for data protection. Prescribed drugs are coded based on the Anatomical Therapeutic Chemical (ATC) classification issued by the European Pharmaceutical Market Research Association.18 Diagnoses are coded to the International Classification of Disease (ICD) version 10 codes.19 Quality of the data is continuously monitored by IMS based on a number of quality criteria (e.g. completeness of documentation, linkage of diagnoses and prescriptions). The validity of IMS DA data has been described previously.20 The database has been widely used in paediatric pharmaco-epidemiological studies in recent years.21–23
Data obtained from the database are anonymous, thus ethics committee approval was not needed for this study.
Study population
The study population comprised all females in IMS DA aged 12–18 years who had at least one prescription for a contraceptive drug (ATC code: G03A) between 1 January 2002 and 31 December 2011.
Study outcomes
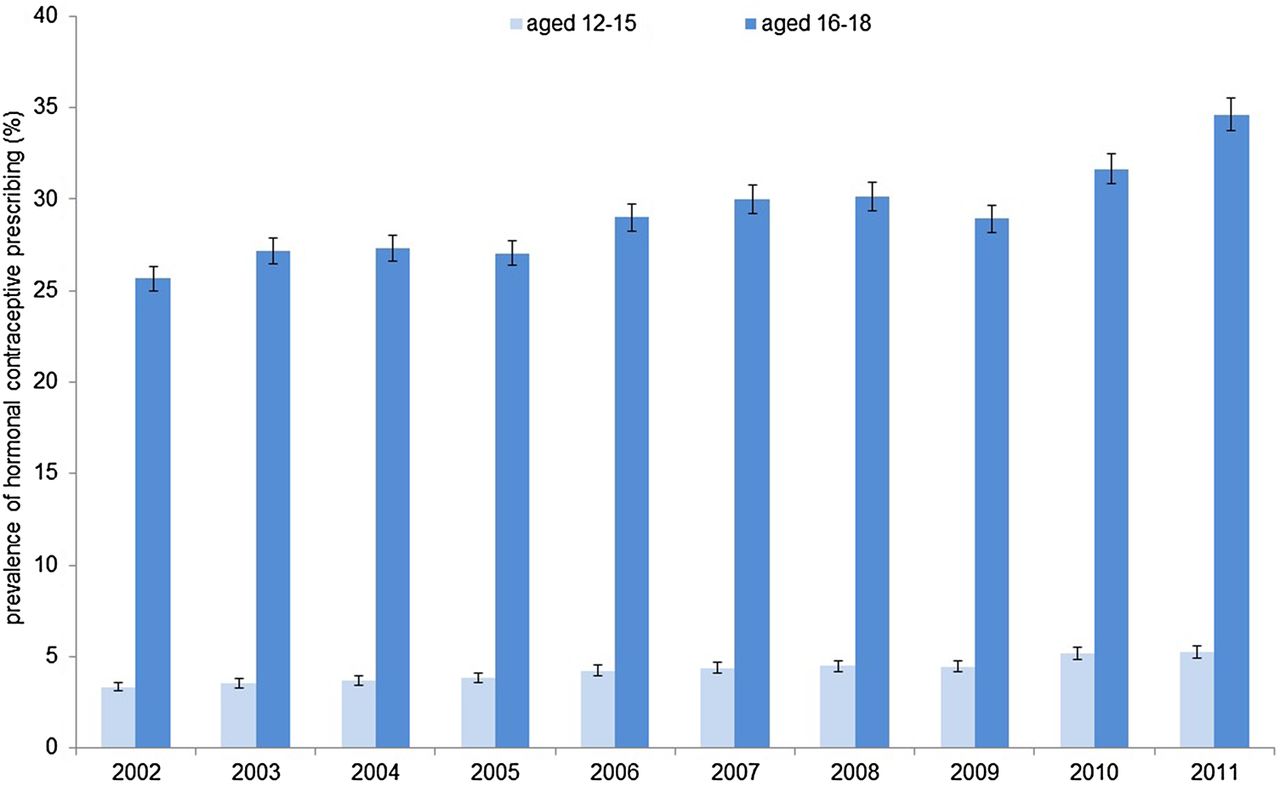
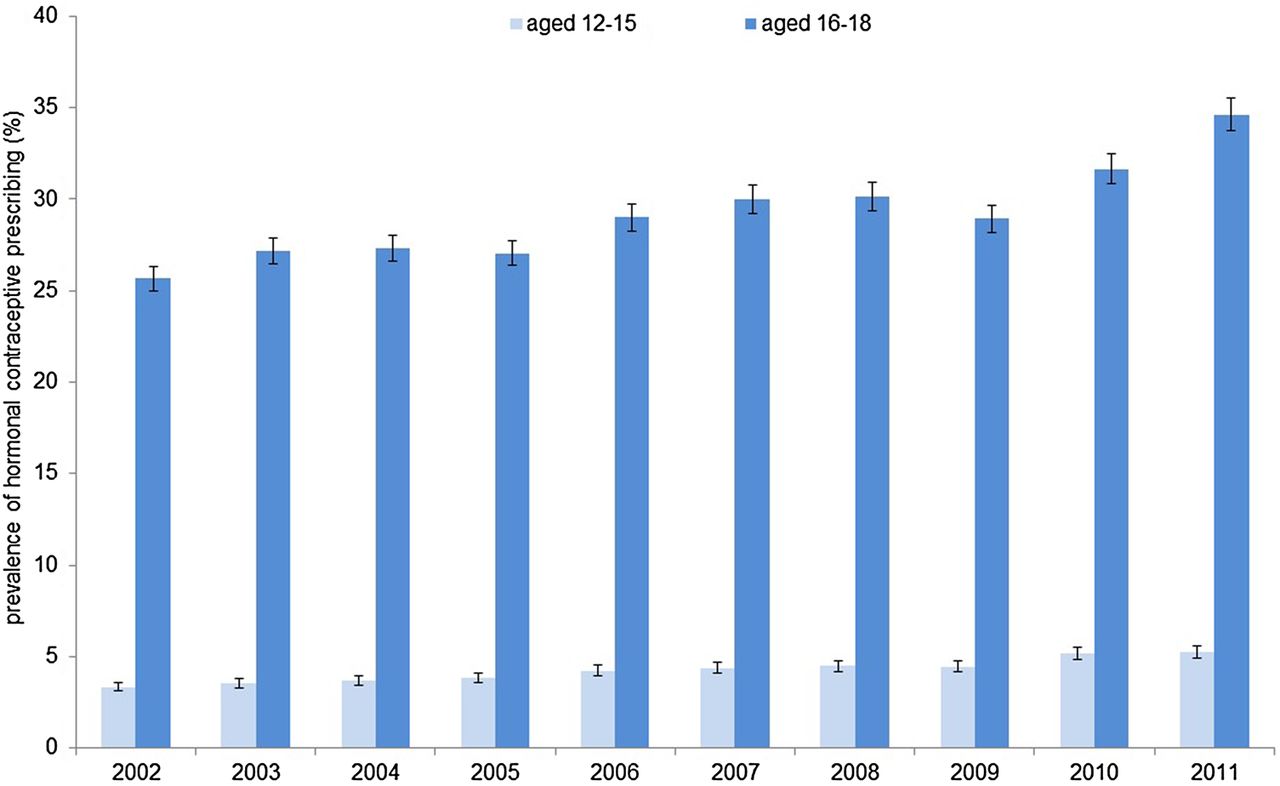
Annual prevalence of contraceptive prescribing was calculated by counting all patients with at least one contraceptive prescription in a particular year, divided by the total number of female individuals in the IMS DA in that year. Annual prevalence of contraceptive drug prescribing was also calculated by age group, defined as those aged 12–15 years and those aged 16–18 years in the relevant year, and expressed as a percentage. Indications for prescribing hormonal contraceptives and the different types of hormonal contraceptives were examined in this population for 2002 and 2011.
The prevalence was calculated for each year for both age ranges, but we have presented the prevalence for 2002 and 2011 only, to show the trends over this 10-year period.
Statistical analysis
Statistical analyses were performed using SAS software V.9.2 (SAS Institute, Cary, NC, USA). Absolute and relative frequencies for contraceptive use by age group and year were calculated. Annual and age-specific prevalence of contraceptive prescribing was calculated using Poisson distribution with a 95% confidence interval (CI).
Results
In total, 44 532 female adolescents aged 12–18 years were identified in the database in 2002 and 34 676 in 2011. In 2002, 13.7% of the female adolescents (n=6135/44 532) received prescriptions for hormonal contraceptives, compared with 19.0% (n=6597/34 676) in 2011. Table 1 shows the patient characteristics and prevalence for prescribing hormonal contraceptives by age group in 2002 and 2011. Figure 1 shows the annual prevalence of contraceptive prescribing by age group between 2002 and 2011. The prevalence of contraceptive prescribing was higher in ages 16–18 years compared to ages 12–15 years (p<0.001). In the 12–15 years age group the annual prevalence of prescribing increased from 3.3% (95% CI 3.1–3.6%) in 2002 to 5.2% (95% CI 4.9–5.5%) in 2011. The annual prevalence of prescribing to those aged 16–18 years increased from 25.7% (95% CI 25.0–26.3) in 2002 to 34.6% (95% CI 33.7–35.5) in 2011.
Characteristics of study subjects in 2002 and 2011, by age group
{kind=link}
Age-specific prevalence of contraceptive drug prescribing by year (with 95% confidence intervals) in general practice in the UK, 2002–2011.
Table 2 shows the indications for prescribing hormonal contraceptives to female adolescents, by age group. The main indication for prescribing hormonal contraceptive drugs was ‘contraceptive management’. In 2002, overall, 76.2% (n=4676/6135) of patients received hormonal contraceptives for this indication compared to 65.7% (n=4334/6597) in 2011. The second most common indication for prescribing these contraceptive drugs in this study population was the treatment of ‘excessive, frequent and irregular menstruation’. The number of female adolescents who received contraceptives for the treatment of acne or urinary system disorders was low. For 8.5–15% of patients the indication was not specified.
Recorded diagnosis for contraceptive prescribing amongst female adolescents in 2002 and 2011, by age group
Table 3 shows the most commonly prescribed hormonal contraceptive formulations by age groups and by year. The COC group ‘progestogens+estrogens’ were the dominant contraceptives used over the study period, of which the combination of ‘ethinylestradiol+levonorgestrel’ was the most frequently prescribed in both age groups; 12–15 years and 16–18 years. Although the usage of progestogen-only contraception was lower compared to COCs, the numbers of patients who received desogestrel and etonogestrel steadily increased in both age groups during the study period, but for levonorgestrel, they decreased. DMPA was the only parenteral progestogen used in our study subjects. There were no prescriptions for vaginal or transdermal contraceptives.
Use of different formulations of hormonal contraceptives for female adolescents aged 12–18 years in general practices in the UK
Discussion
This study investigated the contraceptive prescribing trends and prescription patterns for female adolescents in the UK primary care setting. The most commonly prescribed formulation was combined oral hormonal contraceptives. This is consistent with the study conducted by Sturkenboom et al.24 in three European countries, which found that, in the UK, oral contraceptives were among the top five drugs prescribed for the genitourinary system.
Our study showed that there was an increase in the prevalence of prescribing hormonal contraceptives by GPs to females aged 12–18 years between 2002 and 2011, and there was an increase in the prescribing of progestogen-only contraceptives (desogestrel, etonogestrel) to females aged 12–18 years during the study period. This might partly explain the decrease in conception rate in women under 18 years as published by the Office for National Statistics in the UK.4 Also, the increased prescribing of hormonal contraceptives might indicate that there has been an increased awareness of sexual health and contraception among female adolescents following the introduction of the UK government's Teenage Pregnancy Strategy.3 Contraceptive management was the main indication for prescribing hormonal contraceptives to our study subjects.
The increased use of progestogen-only contraceptives might be because they do not increase the VTE risk significantly compared to COCs.25 Conversely, the prescriptions of levonorgestrel decreased over the years, particularly in the younger age group. One possible explanation might be related to the potential increased efficacy of the desogestrel progestogen-only pill (POP) with its 12-hour rule for missed pills, compared to the levonogestrel POP with the need for greater compliance due to loss of efficacy if a pill is taken more than 3 hours late.26 Levonorgestrel is also prescribed as an emergency hormonal contraceptive in the UK,27 thus the amount prescribed might suggest that it was prescribed for that purpose, though this is not specified in the database. Another explanation might be that since 2001 emergency hormonal contraceptives can be obtained from community pharmacies in the UK by those aged over 16 years,28 thus their data in the GP records may have decreased.
Our study has shown that hormonal contraception prescribing steadily increased between 2002 and 2011. The usage of hormonal contraception was higher in girls aged 16–18 years compared to girls aged 12–15 years. This is consistent with a recent retrospective study from Germany that investigated the prescribing trends of contraceptives in adolescent girls in 2007 and 2011. This study also found a significant increase in contraceptive usage among this population29 that may indicate that the older teenage girls became more concerned about unwanted pregnancy. Another possible reason for less contraceptive prescribing to the younger age group could be that a lower proportion of them were sexually active.30 ,31 However, previous studies have reported that concerns about contraceptive side effects might lead younger girls to discontinue or avoid using contraceptive pills, which could increase the risk of unintended pregnancy.7 ,32 ,33
VTE has been associated with the use of combined hormonal contraceptives.31 A recent review reported that COCs containing desogestrel, gestodene or drospirenone, in combination with ethinylestradiol, are associated with a higher risk of VTE compared with other contraceptives.34 There remains a debate about the VTE risk associated with the use of contraceptive pills but we cannot comment on this potential association in female adolescents, as it was not possible to investigate this in our current study. Further research is needed to investigate this association in this age group.
A range of contraceptive formulations was prescribed to our study population. The most commonly prescribed preparation was the COC containing ethinylestradiol+levonorgestrel. This is consistent with the results from studies in adult women.31 The use of DMPA, which was the only injectable contraceptive used by our study population, was very low over the study period. This may be because DMPA has been associated with bone mineral density reduction in women aged 12–18 years.3 Whilst some data suggest that there may be substantial increases in bone mass after DMPA is stopped,7 information on long-term follow up after discontinuation of use in those women is still lacking.
Study strengths and limitations
To our knowledge, this is the first population-based study to investigate prescribing patterns of hormonal contraceptives to female adolescents in the UK in the general practice setting. Our study has provided comprehensive information on the prescribing trends and patterns of hormonal contraceptives to female adolescents from 2002 to 2011. Also, the database used in this study provided data to enable us also to investigate the indications for prescribing these contraceptives to teenagers and the formulations used.
However, this study has several limitations. First, the database only contains prescriptions issued in the primary care setting, and excludes those prescribed or supplied from family planning clinics or hospitals. However, the number of prescriptions from these sources is expected to be small because the majority of contraceptive prescriptions for adolescents are issued by GPs.36
Second, the IMS DA does not contain data on ethnicity and socioeconomic status, thus their impact on contraceptive use in female adolescents could not be investigated. Finally, there was no information in the database on compliance and adherence to prescriptions issued. This is a general limitation of many health care databases as they contain information on prescriptions issued but do not contain information on whether the prescription was dispensed, nor whether it was taken.
Future research
The use of hormonal contraceptives in female adolescents increased from 2002 to 2011, but there is little, if any, information on the long-term safety of these drugs in adolescents, in particular for girls aged under 16 years. The UK continues to have the highest teenage pregnancy rate in Europe. As younger adolescent girls who are sexually active were found to be three times more likely to become pregnant than those who have sexual intercourse for the first time aged over 16 years,37 there is a need to prioritise research into contraceptive drug use in female adolescents, especially for those aged under 16 years. The recent PRAC review concluded that the benefits of reducing unwanted pregnancy outweigh the risk of VTE for all hormonal contraceptives, but as knowledge on the long-term safety of contraceptive use in adolescents is limited, continued monitoring of their use in this group is warranted.
Conclusions
We found an increase in the prescribing of hormonal contraceptives to female adolescents in the UK from 2002 to 2011 for both the 12–15 and 16–18 years age ranges. As there is little, if any, information about the long-term safety of the use of hormonal contraceptives in adolescents, further research is needed.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Highlights from this issue