Article Text

Abstract
Background and objective:Chlamydia trachomatis infection is a common sexually transmitted infection with serious sequelae. Excellent access to testing, treatment and contact tracing are an essential part of strategies to control it. With traditional sexual health services overstretched, community pharmacies are well placed to provide this service. They have the potential to improve access by offering chlamydia testing and treatment from high street venues with long opening hours. This study evaluated the feasibility and acceptability to users and pharmacists of this service in independent community pharmacies.
Method: A chlamydia testing and treatment service was offered in three community pharmacies in two inner London boroughs for a 3-month pilot. Data on the feasibility and acceptability of the new service were collected via a survey of client experience, indepth semistructured interviews with clients and pharmacists, and structured evaluation reports completed by professional patients paid to visit the pharmacies.
Results: 83 tests were taken with eight (9.5%) of these positive for C trachomatis. Of those tested, 94% (n = 73) were women and 71% (n = 56) were from ethnic minorities. 80 clients completed the questionnaires and 24 clients were interviewed. Most clients heard about the service from the pharmacist when requesting emergency contraception and 16% (n = 13) would not otherwise have been tested. Clients valued the speed and convenience of the service and the friendly, non-judgmental approach of the pharmacist. Confidentiality when asking for the service at the counter was suboptimal, and the pharmacist trained to deliver the service was not always available to provide it.
Conclusions: Chlamydia testing and treatment in community pharmacies is feasible and acceptable to users. The service increases access among young women at high risk of sexually transmitted infection but not among young men.
- Poster prize winner:, This paper was commissioned after winning first prize for posters at the 2006 International Forum on Quality and Safety in Health Care, in Prague
Statistics from Altmetric.com
Community pharmacists have an increasingly important role in sexual healthcare. Many provide emergency contraception,1 pregnancy tests, condoms,2 treatment for vaginal candidal infection2,3 information on hepatitis B and HIV,4 and sexual health promotion.5 Community pharmacists are therefore potentially well placed to offer testing and treatment for genital Chlamydia trachomatis infection.
C trachomatis infection is the commonest sexually transmitted infection diagnosed in the UK and its incidence is increasing, particularly among young people.6 It is often asymptomatic and may have serious sequelae such as subfertility and ectopic pregnancy.7 An essential element of chlamydia control strategies is testing for this infection, with treatment and contact tracing of positives.8 This has been traditionally provided by sexual health services and general practice. Other providers are being considered since existing providers are overstretched9 and the stigma associated with sexual health service use limits service uptake in this setting.10,11
In the UK, a national pilot of chlamydia testing was launched in November 2005 in a large high street pharmacy chain (Boots).12 A local audit in the London boroughs of Lambeth and Southwark generated new data showing that small community pharmacists are important providers of sexual health services (Lambeth and Southwark Sexual Health Modernisation Programme, unpublished report, 2005). Small community pharmacies are used for medical prescriptions by about half of the UK population and are used by a population different from that using the high street pharmacy chains.13 We piloted the provision of a chlamydia testing and treatment service in independent community pharmacies to test its feasibility and acceptability in this setting.
The present study aimed to assess the feasibility of the community pharmacy led Chlamydia testing programme and to evaluate uptake and client/practitioner satisfaction with this method of service delivery.
METHOD
A chlamydia testing and treatment service was set up at three independent community pharmacies in the London boroughs of Lambeth and Southwark. These pharmacies were selected from those that were eligible because of their location. We intended the pilot to cover as much of the two boroughs as possible. The pharmacists were experienced providers of emergency contraception and received additional training on C trachomatis infection. The pharmacies and the local sexual health clinics advertised the service. Those with positive tests and their contacts received treatment under a patient group direction, and partner notification was user-led. The King’s College Hospital research ethics committee approved the study.
For testing the feasibility and acceptability of this service we carried out a questionnaire survey of the clients, and indepth semistructured interviews with the clients and pharmacists. The laboratory that tested the specimens provided data on the number of samples tested and the rate of positivity, and the pharmacies were evaluated by professional patients.
For the user survey all those requesting chlamydia testing were invited to complete a questionnaire by the pharmacist at the end of the consultation (box 1). The questionnaires were developed on the basis of consultation with users of sexual health services on the attributes of high-quality sexual health services. Data on the age, sex and ethnicity (based on self-classification in relation to UK census categories) of each user was also obtained through the questionnaire survey. Completed questionnaires were placed by the client in a sealed, stamped, addressed envelope and posted by the client or pharmacist to the research base.
Box 1: Topics covered by the questionnaire for service users
The questionnaire included closed questions on:
-
Source of information about the service
-
Relationship to the pharmacy (local pharmacy or usual pharmacy)
-
Alternative sources of testing considered
-
Previous sources of advice on sexual infections
-
Adequacy of privacy in pharmacy
-
Preferred source of treatment if result positive
-
Additional services obtained from pharmacy at same visit
-
Preferred type of pharmacy as source of chlamydia test (high street chain or independent)
-
Demographic details and Likert scales to indicate client satisfaction and level of comfort discussing sexual health with the pharmacist
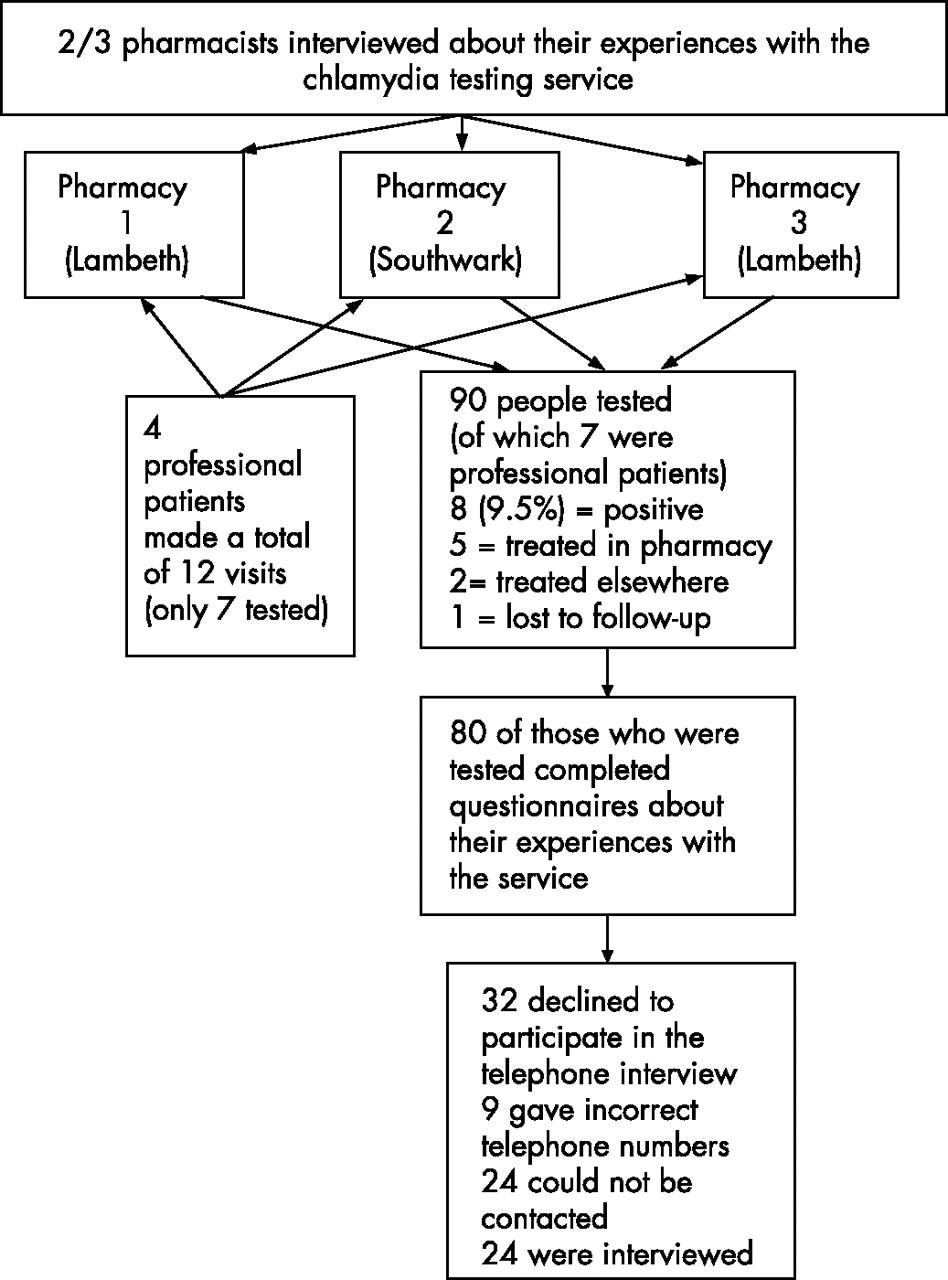
Of the 83 tests taken (excluding seven to professional patients) eight (9.5%) were positive. Five of the participants with the positive tests were treated (fig 2) in a pharmacy, two were treated elsewhere and one was lost to follow-up. For those treated in a pharmacy the average time between testing and treatment was 4.6 days.

Participant recruitment details, September to November 2005.

{kind=link}
{kind=link}
Protocol for testing and treatment. *Includes tests offered to professional clients; **excludes professional clients’ tests.
At the time of service use clients were invited to discuss their experience of testing. Those who accepted subsequently underwent a short, semistructured (15–30 min) interview on telephone. Qualitative data on the experience of service provision were also available from two of the three pharmacists who participated in a semistructured telephone interview on their experience of service provision. The interviews with both users and pharmacists were recorded in note form during the interview.
To test the correct implementation of the programme, professional patient evaluators visited the participating pharmacies on three occasions each. Professional patient evaluators are trained service users employed to visit and evaluate clinics without revealing their identity. The evaluation questionnaire completed by the professional patients included closed and open questions on each stage of the visit.
Analysis
The numerical data are presented as frequencies and percentages. Two researchers independently coded the data and identified key themes from the telephone interviews with users and the interviews with the community pharmacists. Within these themes hypotheses were generated and the data were searched for material that contradicted these with each hypothesis rejected or modified accordingly. In addition, simple counting was used to give an indication of the extent of the support for each theme within the data.14 The two researchers then compared their analysis and resolved any differences. The quantitative data from the 12 professional patient reports were entered into a spreadsheet and analysed using SPSS (v 13), and the qualitative data were analysed thematically as above. For the purpose of this paper participants have been given pseudonyms.
With regard to the telephone interviews, 32 clients declined to participate, 9 gave incorrect telephone numbers, 24 could not be contacted and 24 were interviewed (fig 1).
RESULTS
During the 3-month pilot, 90 chlamydia tests were done. Seven of these were taken by professional patients and have been excluded from the analysis. On six occasions the professional patients tried to access a test but the trained pharmacist was unavailable. In all, 80 questionnaires were completed (96% response rate), excluding those completed by the mystery shoppers; 94% (n = 73) were completed by women and five by men. Just over half of users were under 25 years of age and 71% were of minority ethnicity.
Most clients (n = 44, 55%) heard about the service from the pharmacist. Half (12/24) of the telephone interview respondents and 49 (60%) of the questionnaire respondents were offered a test when they requested emergency contraception.
“I went to get emergency contraception. He [the pharmacist] said you could take a chlamydia test. I hadn’t heard about it.” (Nuala)
Thirteen (16%) of the questionnaire respondents reported that without this pilot they would not have been tested while the rest would have requested a test elsewhere (48% from a sexual health service and 29% from their general practitioner(GP)). Forty-eight (60%) of questionnaire respondents were tested in a pharmacy local to them and 33 (41%) at the pharmacy they regularly used.
With regard to the service, 64 (80%) of questionnaire respondents were “very satisfied” and 11 (14%) were “satisfied”. All felt “very comfortable” or “comfortable” discussing sexual health with the pharmacist and 76 (95%) found the consultation was sufficiently private. The telephone interviews confirmed the confidentiality of the consultation but identified concerns about confidentiality at the counter.
“There were other people around—no queue. A bit embarrassing but just had to do it.” (Ella)
Clients felt it was appropriate to discuss sexual health issues with their pharmacist.
“He was approachable and professional ... it doesn’t matter whether he or she is not a doctor or a nurse as long as they are professional in their approach.” (Nazreen)
The excellent communication skills of the pharmacists (19 comments) and counter staff were important to respondents.
“Nice people … pharmacist was easy to talk to … polite, wasn’t giving me looks or anything. I thought he was honest.” (Suzanne)
The pilot created some additional business for the pharmacists with two users picking up an additional prescription during their visit and five purchasing an item, but it generated few new visits. Of the questionnaire respondents, 75 (91.5%) would prefer to return to the pharmacy where they had been tested for treatment.
In all, 72% preferred to access the service at an independent pharmacy rather than a large pharmacy chain and 23.2% had no preference.
“Small pharmacy is more personal, more committed to what they are doing … it’s their life.” (Jo)
The telephone interview respondents liked the short waiting times (n = 10), drop-in service (n = 2) and anonymity (n = 7). When asked whether the community pharmacy is an appropriate place to provide chlamydia testing, 18 felt it was and all would recommend the service to a friend.
“Yes because it makes it easier. I’ve been wanting to get it done for ages. I went to my clinic but you have to ring up and make an appointment and I just never got that far. So when he said they did it I was really pleased.” (Kath)
“They [community pharmacies] are a lot more convenient ... at least you know that they are open from the morning to the evening. Clinics are different times.” (Megan)
The professional patients reported difficulty accessing the service when they needed it. Professional patient evaluators could not obtain a test on their first attempt in seven of their visits. In six instances this was because the pharmacist trained to take the test was not available. Visits where tests were obtained took an average of 22 min (range 8–35 min). All professional patients found the counter staff polite and most waited less than 2 min at the counter. Five could be overheard at the counter and two felt they had been asked inappropriate questions at this stage. But they were impressed by the friendliness of the reception, and all of the professional patients found the pharmacists friendly and non-judgmental.
“The girls at the counter were very pleasant and polite. They did ask me tactfully if I could tell them why I needed to see the pharmacist but I said it was confidential ...” (Elaine)
The professional patients described the strategies employed by pharmacists to manage both the more complex chlamydia consultations as well as the routine pharmacy business:
“The pharmacist was obviously busy and kept coming and going as he had to keep an eye on the other member of staff.” (Elaine)
“The pharmacist was very busy and understaffed. Due to this he was on the phone for some time. However, he seemed to make it a priority that I had a chair to sit on and was comfortable. Due to being understaffed I had my consultation at the back of the shop rather than downstairs in the consultation room. However, this was only after he had asked my permission for this.” (Ahmed)
The two pharmacists interviewed enjoyed the pilot and felt the sexual health training built confidence and skills. Both were nervous at the start of the pilot.
“Initially I thought ‘Am I going to be inundated? Have we bitten off more than we could chew?’” (Pharmacist A)
Although they agreed that:
“Once you’ve done a few and got confidence it takes much less time.” (Pharmacist B)
They felt that good advertising was essential—particularly for men. A chlamydia test alongside emergency contraception saved women the time and embarrassment required to use other services.
“Some of them nearly tried to kiss you! In our place it’s much nicer and in clinics everyone sits and looks at you, you feel judged. If you see your GP you worry it could end up on your records. With us it’s confidential so they can tell you all you need—sometimes even more than you need!” (Pharmacist B)
The opportunity to provide testing and treatment did seem to fit in the pharmacist’s role.
“We can be more effective. Not just talking about something, we can do something ... and if people care for themselves they won’t go to their GP unnecessarily.” (Pharmacist A)
It also gave a sense of pride and fulfilment.
“You feel like a professional. It’s morally satisfying that you’re providing a proper service.” (Pharmacist B)
All the pharmacists said they would continue to provide the service and would strongly recommend that other colleagues to try the scheme if paid for the time required for the consultation and associated paperwork. Further research is required to compare community pharmacy testing with the cost of existing services.
DISCUSSION
Chlamydia screening in community pharmacies seemed feasible and acceptable to pharmacists and service users in two inner London boroughs with high levels of sexual ill health. The pilot effectively reached young women from ethnic minorities and those accessing emergency contraception, both groups known to be at high risk of sexually transmitted infection.15,16 However the actual incidence of infection (9.3%) was lower than that recorded in family planning clinics and general practice locally (12.7% women; 19.1% men). The pilot did not reach young men, a group that has been consistently hard to reach. In the UK national chlamydia screening programme the uptake among men is 12.5%17 and in the first year of the national pilot in Boots (a large high street pharmacy chain) 21% of those tested were male.12 The low numbers of men tested in this pilot may be because most clients heard about the service from a pharmacist during a consultation for emergency contraception.
The provision of chlamydia testing in community pharmacy seemed to increase access to testing among those who would not otherwise have been tested and could potentially reduce demand in other sexual health services. Users valued the convenience in terms of proximity to home, predictable opening hours, no waiting and not having to make an appointment. The respondents in the present study were happy to discuss sexual health with their pharmacist, and both users and professional patients were impressed with the friendly approach from counter staff. This contrasts with reports from users and the same professional patients on sexual health services that identify unfriendly receptionists and to a smaller extent unfriendly medical and nursing staff as a problem.18
Our results do not suggest the pilot increased business for the pharmacists involved. Most of those using the service would have visited the pharmacy anyway and few made additional purchases. The benefits for pharmacists of providing this service include greater skills training and job satisfaction, increased sales of other products, greater customer satisfaction and return visits.
This paper adds to early reports from the national pilot in which the client questionnaire return rate has been exceptionally low and no qualitative data from service users or pharmacists were published.12 Data on client experience of chlamydia testing in community pharmacy is an important element of the evidence to inform decisions on the maintenance and possible expansion of this programme.
Limitations of this study
The study would benefit from data on the number of contacts treated per case of chlamydia and cost comparisons between venues for testing. This is a very small pilot with only 90 tests across three pharmacies over 3 months. It is well known that pilots of this sort benefit from the commitment and enthusiasm of those involved and the results may not be generalisable on a larger scale. Uptake of the service was low with an average of only 10 tests a month per pharmacy. It is unclear whether this was due to the limited availability of the pharmacist trained to provide this service, as shown by the professional patient evaluators, poor advertising—most users heard about the service during an emergency contraception consultation—or lack of demand for this service in pharmacies.
CONCLUSION
Community pharmacies are a suitable location for chlamydia testing and treatment. Further work is required to encourage uptake by young men and improving confidentiality at the counter.
Demographic details of people tested for chlamydia in the community pharmacy pilot
How did participants hear about the chlamydia testing service?
Acknowledgments
We would like to thank Beth Taylor for her support throughout this project.
REFERENCES
Footnotes
-
Funding: The Lambeth and Southwark Sexual Health Modernisation Programme is funded by the Guys and St Thomas’ Charity to redesign sexual health service provision in partnership with service users and providers to better meet the needs of the local population. This project was funded by the Guys and St Thomas’ Charity.
-
Competing interests: None declared.