Article Text

Abstract
Throughout the latter half of the 20th century, hormone-replacement therapy (HRT) use steadily increased in the Western world. In 2002, the early termination of the Women's Health Initiative trial due to an excess of adverse events attributable to HRT, led to a precipitous decline in its use. Breast cancer incidence began to decline soon thereafter in the USA and several other countries. However, the magnitude of the decline in breast cancer incidence, and its timing with respect to HRT cessation, shows considerable variability between nations. The impact of HRT cessation appears most significant and immediate in countries with the largest absolute decline in HRT use. In countries in which peak prevalence of HRT use was high, several studies have convincingly excluded decreasing rates of mammographic screening as an explanation for the decline in breast cancer incidence. Conversely, in some countries, no decline in breast cancer incidence is apparent that can be readily attributed to declining trends in HRT use. In such cases, declines in breast cancer incidence may be related instead to saturation or decreased utilisation of mammographic screening programmes. In other cases, it is difficult to disentangle the respective influence of trends in HRT use, and the influence of changes relating to mammographic screening. However, irrespective of time lags and varying magnitudes of effect, the data convincingly support a direct association between decreasing HRT use and declining breast cancer incidence.
- Breast neoplasms
- hormone-replacement therapy
- incidence
- trends
- populations
- cancer epidemiology
- cancer: breast
Statistics from Altmetric.com
- Breast neoplasms
- hormone-replacement therapy
- incidence
- trends
- populations
- cancer epidemiology
- cancer: breast
A brief history of hormone-replacement therapy use
The use of hormone-replacement therapy (HRT) dates back to the late 19th century, when treatment of the ‘climacteric’ included oral preparations of pulverised cow ovaries.1 The discovery in the 1920s of high levels of oestrogen in the urine of pregnant women lead to the successful commercialisation of oestrogen isolated from the urine of pregnant mares (most notably Premarin©) in the early 1940s.1 The use of HRT to treat symptoms of menopause continued to increase steadily thereafter. This rise was fuelled by numerous observational studies published in high impact medical journals, which strongly suggested exogenous HRT was associated with a large and significant reduction in coronary heart disease and death among apparently healthy women.2 Ironically, early warning signs of the adverse cardiovascular effects of hormonal therapy from its use in men in the coronary drug project randomised trial were ignored, as the use of HRT in women continued to rise.3 Thus ‘despite nature's designs, the management of menopause became increasingly “medicalised”, such that many considered HRT to be physiologic, and its use preventative against cardiovascular disease’.4 The belief in the health benefits of HRT was widely held; a survey of female physicians in the 1990s found that almost 30% of them were personally using HRT solely for disease prevention.5 As discussed in subsequent sections, results from the Women's Health Initiative (WHI) randomised trials of HRT use, published in 2002, subsequently dispelled many of these beliefs, demonstrating a significant increase in coronary heart disease, stroke and venous thromboembolism, and an increased risk of breast cancer associated with HRT. The WHI findings subsequently lead to a rapid decline in HRT use in many countries. The ‘rise and subsequent fall of HRT use’ is illustrated in figure 1.
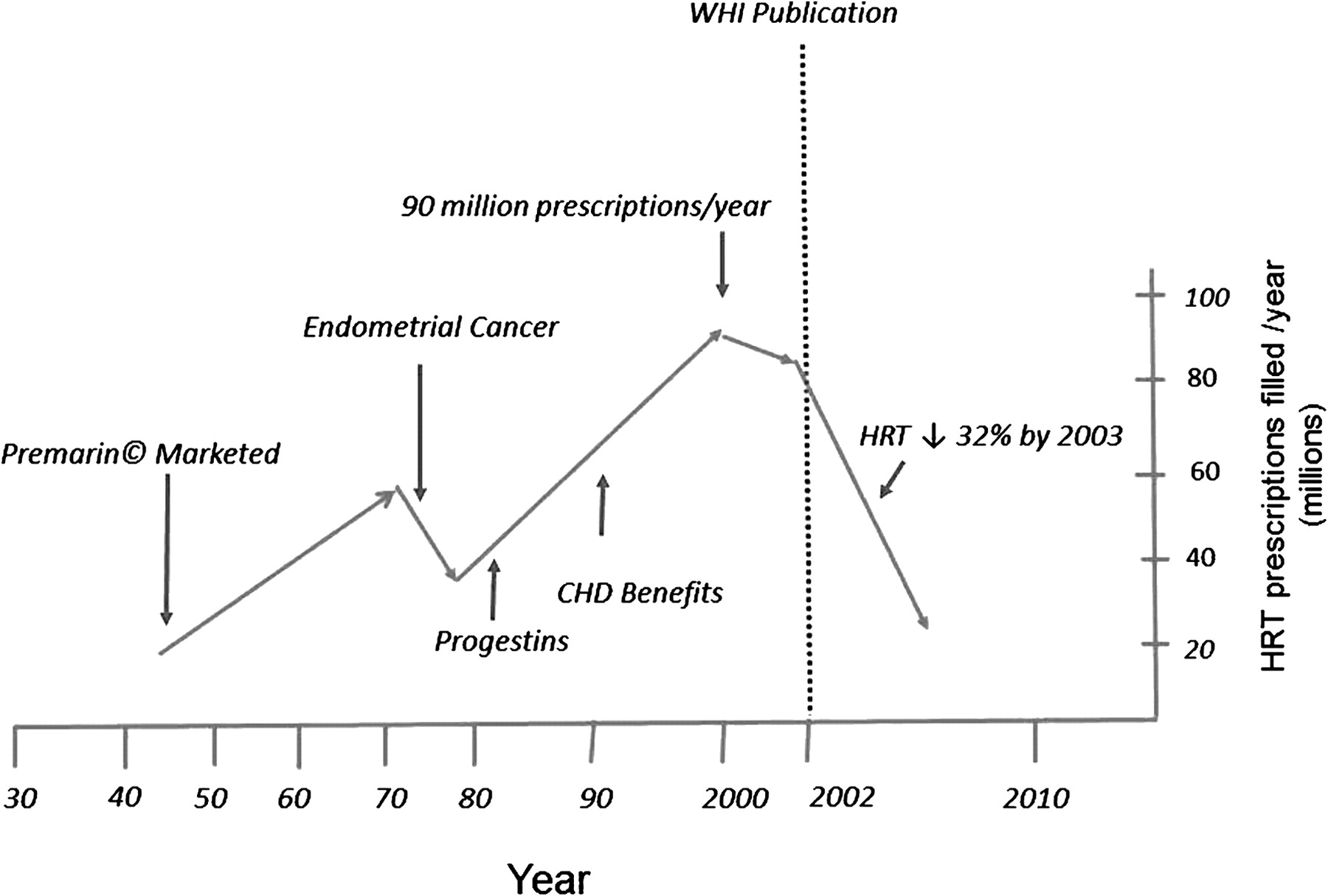
Trends in hormone replacement therapy (HRT) use (all formulations) over time in the USA.1 7 8 9 Endometrial cancer: oestrogen monotherapy is associated with an increased risk of endometrial cancer. Progesterone: the addition of progestins to oestrogen eliminates excess risk of endometrial cancer. Coronary heart disease (CHD) benefit: Purported benefits of HRT with respect to prevention of coronary heart disease.
Observational data linking HRT use to breast cancer risk
Prior to the WHI results, observational studies examining HRT use and breast cancer risk were inconclusive. However, the Collaborative Group on Hormonal Factors meta-analysis of many of these studies, published in 1997, demonstrated a statistically significant increase in breast cancer associated with HRT use of more than 5 years duration (RR=1.35), with longer durations of use associated with even higher risk.10
WHI trials
The WHI trials consisted of a series of randomised trials and a large observational study, designed to examine multiple outcomes including breast cancer incidence (table 1).
The Women's Health Initiative (WHI) trials11
The WHI randomised trial of oestrogen and progesterone (EP) versus placebo was the pivotal trial demonstrating an increased risk of breast cancer associated with HRT use.6 The EP trial was stopped early after demonstrating an excess risk of venous thromboembolism, coronary heart disease, stroke and breast cancer among those receiving HRT.6 The RR of breast cancer was 1.24 (95% CI 1.02 to 1.55) compared to placebo, and increased with duration of exposure. In contrast, the WHI randomised trial of oestrogen monotherapy versus placebo in women with prior hysterectomy did not demonstrate an increased risk of breast cancer.1 In addition to these randomised trials, the WHI observational study reported breast cancer incidence data on 25 328 women who did not use HRT and 16 121 who reported use of EP.12 In the EP cohort, the estimated HR for breast cancer was 2.0 compared with non-users.
The Million Women study and the influence of HRT preparation
The Million Women observational study examined the association between HRT use and incidence of breast cancer among 1 million women aged 50–64 from the UK from 1996 to 2001.13 Approximately half of the women had used HRT at some point, with approximately 30% current HRT users during the study period. There was an increase in breast cancer risk in current users of HRT (RR=1.6), that increased with duration of use. Importantly, there were no significant differences in risk associated with different routes of HRT administration, specific form of HRT used, or HRT dose. In contrast, other studies have suggested that HRT preparation type is relevant.14 Since it is unclear whether breast cancer risk varies among different HRT preparations, this article will not explore the potential impact of differences in HRT preparation use between countries.
The prevalence of HRT use prior to the WHI publications
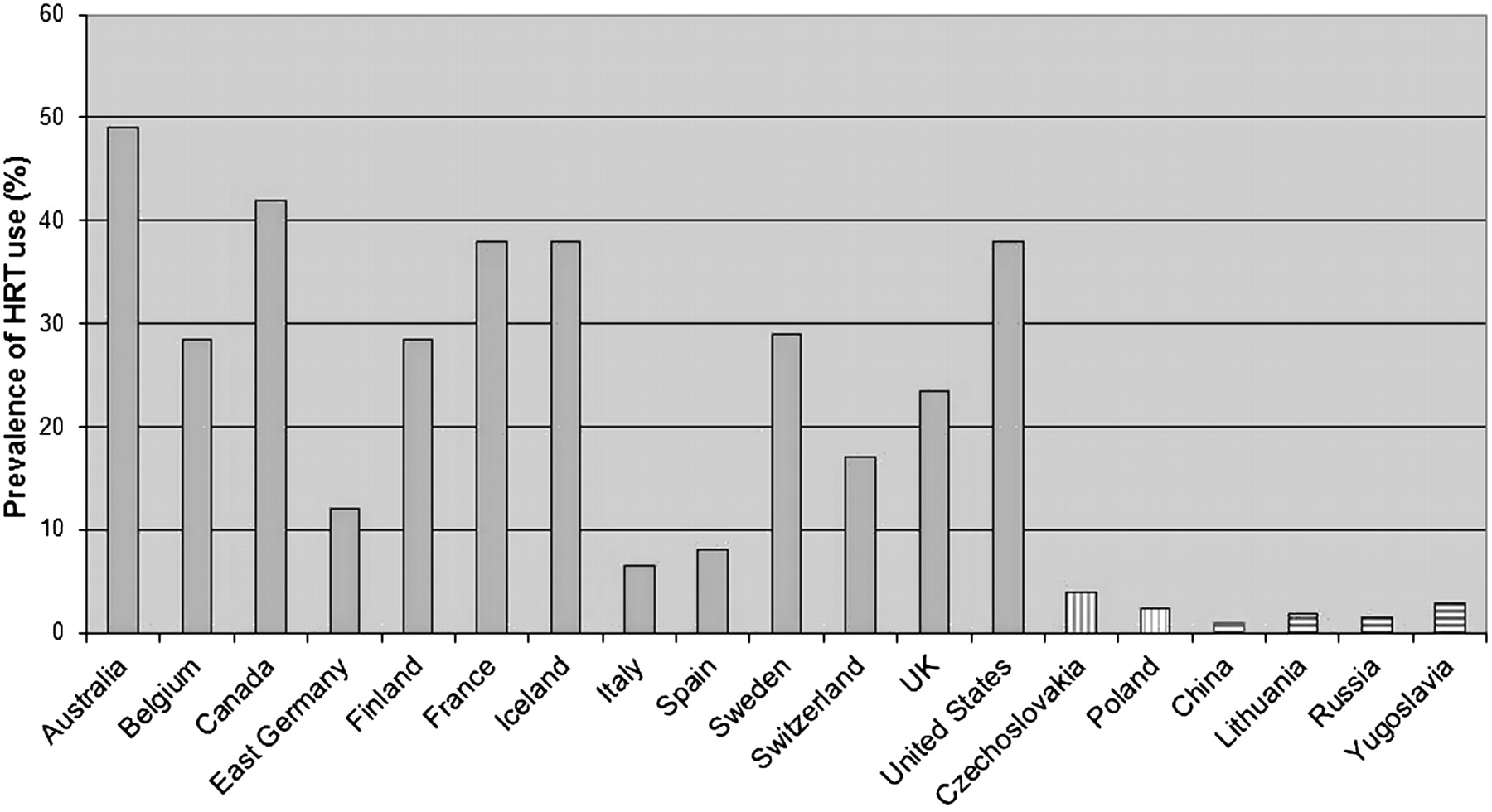
Although studies from the USA have reported somewhat variable rates of HRT use, Hersh et al estimated HRT use at 33% in 1995 and 42% in 2001,7 and similar figures have been reported in other studies.15 16 Globally, peak HRT use varied dramatically; the percentage of women reporting ‘ever use’ of HRT use was 1.8% in Indonesia, 20.2% in Latin American countries, 38% in Europe, and 43% in the USA.17 The Monitoring of Trends and Determinants in Cardiovascular disease (MONICA, WHO) project confirms this global variability; HRT use was highest in North America, Australia and much of North-Western Europe, while in China and Eastern Europe use was markedly lower (figure 2).18 Not surprisingly, the countries with the highest prevalence of HRT use are all classified as high income by the World Bank.19 As discussed in detail in subsequent sections, variability in peak HRT use is likely one key explanation for why declining HRT use has resulted in different breast cancer incidence trends in different countries.
{kind=link}
{kind=link}
Prevalence of hormone replacement therapy (HRT) use globally in the late 1990s sorted by World Bank Income Classification in the year 2000.18 Solid grey, World Bank high income country; vertical hatches, World Bank upper middle income country; horizontal hatches, World Bank lower middle income country.
The precipitous decline in HRT use after the WHI publication
Publication of the WHI results in 2002 resulted in extensive media exposure, and HRT use declined rapidly in many countries. A US report based on pharmaceutical databases demonstrated a steady rise in HRT use between 1992 and 2002, peaking at greater than 87 million prescriptions annually, with a subsequent decline of 32% to 59 million prescriptions in 2003.8 A California study suggested the decline occurred rapidly; 55% of woman attempted to discontinue HRT within the first 6 months after the publication of the WHI results.20 Similar trends were observed in Canada21 and in several European populations,22 details of which follow in subsequent sections.
The decline in breast cancer incidence in the USA
Data from the SEER (Surveillance, Epidemiology and End Results) registry demonstrated that breast cancer incidence increased 0.5% per year from 1990 to 1998.23 Thereafter, rates remained relatively stable until 2003, when breast cancer incidence decreased 6.7% compared with 2002.23 24 Therefore, a decline in breast cancer incidence occurred almost immediately after HRT use began to decrease. Interestingly, an earlier, more subtle decrease in breast cancer incidence was observed from 1999 to 2000. This decline, also evident in several other countries, is discussed in greater detail later in the article.
A subsequent publication from Northern California found HRT prevalence was 35% in 2001, with a subsequent decline of 68% to 12% by 2003.25 Breast cancer incidence decreased 10% during the same period. A subsequent report compared HRT use and breast cancer incidence between different counties in California.26 The authors hypothesised that the magnitude of the decline in breast cancer in different counties would correlate with regional changes in the use of HRT.26 Counties were stratified based on HRT use in 2001 (low, <15%; medium, 15–20%; and high, >20%). By 2003 there was little difference in HRT use between counties; therefore the absolute decline in use was larger in the high prevalence counties compared with low prevalence counties. Breast cancer incidence declined 8.8% between 2001 and 2004 in counties with the smallest absolute reduction in HRT use, 13.9% in those with intermediate reductions, and 22.6% in counties with the largest reductions. Importantly, between 2001 and 2003 there was no significant change in the proportion of women who reported having a screening mammogram.
Changes in rates of mammographic screening in addition to saturation of screening programmes remain important confounders when examining breast cancer incidence in relation to HRT use. Nationally, rates of screening mammography in the USA decreased by 2% between 2002 and 2003,27 however it is generally felt that this decrease was not large enough to explain the dramatic decrease in breast cancer incidence seen during this time. The potential influence of changes in mammography rates is discussed further in subsequent sections.
An ‘immediate’ decline in breast cancer incidence in other nations
Similar to the USA, several countries have demonstrated declines in breast cancer incidence that occurred soon after HRT began to decrease (table 2). These trends are evident exclusively in high income Western nations, in whom HRT use was historically more prevalent than the rest of the world. Unlike the USA, rates of mammographic screening in several of these countries were increasing significantly during the time when breast cancer incidence was declining, thereby complicating the association between HRT use and breast cancer incidence.
Hormone replacement therapy (HRT) use, breast cancer incidence and mammography rates in countries with an ‘early’ decline in breast cancer incidence after publication of the Women's Health Initiative HRT results in 2002
Germany
In the region of Schlewsig-Holstein in Germany, rates of HRT use before 2002 were comparable to those in the USA.28 There was a 50% decline in HRT use by 2005, and breast cancer incidence decreased 8.8% annually between 2002 and 2005. Regression analysis demonstrated a small decline in 2003 followed by a more pronounced decline in 2004 and 2005. A subsequent publication from cancer registries throughout Germany correlated breast cancer incidence with HRT use from 1997 to 2006.34 There was a very strong correlation between the absolute decline in HRT use and breast cancer incidence among different regions. Regions with the highest use in 2001 had the highest breast cancer incidence in 2002, and subsequently the largest decline in breast cancer incidence thereafter. Mammography rates in many regions of Germany increased during this period, as organised screening programmes matured.
France
Breast cancer incidence began to decline in 2003, decreasing by 14.7% and 12.6% in women aged 55–59 and 60–64 years, respectively, from 2003 to 2007.35 HRT use peaked in 2001 at 32% and decreased to 11% by 2007. This decline in breast cancer incidence occurred during a time period when breast cancers detected by screening mammography were increasing.31
Belgium
In the province of Limberg, HRT use peaked in 2001–2002, with 33% of women aged 55–59 years filling HRT prescriptions.29 By 2005, HRT use decreased by greater than 60%. Breast cancer incidence decreased 9.5% annually from 2002 to 2004. A national breast cancer screening programme was adopted in 2000, and consequently rates of screening mammography increased between 2000 and 2005.
Australia and New Zealand
In Australia, HRT use peaked in 2001 at 21%, and decreased 40% by 2003. Breast cancer incidence decreased by 6.7% in 2003 compared with 2001 in women aged 50 years and older,33 with this trend being sustained in 2005.36 Mammographic screening rates remained stable from 2001 to 2005.36 Very similar trends were observed in New Zealand.37
Canada
HRT use was 30% in 2002, and decreased to 15% by 2004. In women aged 50–69 years, breast cancer incidence decreased by 8% per year from 2002 to 2004.30 Mammography rates were stable from 2000 to 2005.
Changes in the age distribution of breast cancer in relation to HRT use
In the Swiss Canton of Geneva from 1975 to 1989, breast cancer incidence increased with age, with rates among women aged ≥85 years three times higher than those of women aged 50–54 years.32 However, by 1997 incidence was highest among women aged 60–64 years. HRT prevalence was >50% in 1996. This shift in age distribution was independent of method of breast cancer detection. Recent data demonstrates a reversal of this trend, beginning in 2003; during this period rates of HRT use fell by >40%.38 The shift in the peak breast cancer incidence described in Switzerland39 was not evident in the Netherlands (where HRT use was never >10%); rates remained highest in women above 80 years of age from 1989 to 2002.39 Both nations had stable rates of mammographic screening during this period. The reversal of age specific breast cancer incidence trends in Switzerland, and the lack of these trends in the Netherlands, adds further support for a causal link between decreased HRT use and declining breast cancer incidence.
Disentangling the influence of mammography and HRT use in the USA
Much debate about potential confounders, especially rates of mammographic screening, accompanied initial reports attributing the decline in breast cancer incidence to decreased HRT use. Cheblowski subsequently presented compelling data from the WHI trial to support a causal association between HRT use and breast cancer incidence.12 Breast cancer incidence in the EP arm increased steadily during the 5.6 year intervention period, and declined rapidly once EP was discontinued. EP discontinuation was nearly universal and occurred very quickly after study unblinding. After discontinuation, the excess risk of breast cancer in the EP arm declined rapidly, and was no longer significant 2.6 years post-cessation. During the intervention and post-intervention periods, mammography rates were nearly identical in the EP and placebo arms.
The California Teacher's Cohort followed >70 000 women 50 years of age or older recruited in 1996 and 1997. Peak HRT use was high, with approximately 60% of women reporting current HRT use in 2000–2001. By 2006, 64% of women had discontinued HRT. Breast cancer incidence fell in the 2003–2005 reporting period compared to the 2000–2002 period by 26%. By collating individual data on HRT use and breast cancer diagnosis, the authors demonstrated that the decline in breast cancer incidence was limited to past users of HRT; no decline was evident for non-users. Mammographic screening rates were stable throughout the course of the study.
Populations with no breast cancer decline attributable to decreasing HRT use
During the early 2000s, either breast cancer incidence in several countries did not decline despite decreasing rates of HRT use, or a modest decline in breast cancer incidence occurred that was unlikely to be explained by decreasing HRT use (table 3).
Countries with no decline in breast cancer incidence attributable to decreasing hormone replacement therapy (HRT) use
Data from the Netherlands did not demonstrate a decline in breast cancer incidence after 2002 despite a decline in HRT use.40 However, HRT peak prevalence was only 13%. Thus, although HRT use declined by 42% in 2005 compared to 2001, this equates to an absolute decline of only 5%. The authors predicted similar trends for much of Italy and Spain, where prevalence of HRT use was historically low (figure 2). A study from Turin, Italy confirmed this speculation.44 The prevalence of HRT use in this region has never exceeded 15%, and the decline in HRT use after 2002 was only 20%. Although a small decline in breast cancer incidence wasevident from 1999 to 2001 that was attributed to saturation of mammographic screening, there was no decline in breast cancer incidence after 2002. A subsequent publication from several regions in Italy reported steadily increasing breast cancer incidence throughout the 1990s, with a very gradual and modest decline thereafter. For many regions, peak breast cancer incidence correlated strongly with a time period several years after inception of organised mammographic screening programmes, likely representing the mammographic detection of subclinical prevalent breast cancer cases. Peak HRT prevalence was approximately 10% in 2000, with very modest declines in 2001–2004.43 It is reasonable to assume therefore that the trends in breast cancer incidence described may have been more heavily influenced by the development, and subsequent saturation, of mammographic screening programmes than by changes in HRT use. A modest decline in breast cancer was reported in Spain after 2001 in women aged 50–64 years.45 However, HRT use peaked at only 5.9% in 1998, suggesting that trends in HRT use would be unlikely to account for the decline. Conversely, mammographic screening coverage of Spain was >90% by 2001, suggesting that, similar to Italy, saturation of mammographic screening was a more likely explanation. In support of this affirmation, the authors demonstrated that the earliest declines in breast cancer incidence occurred in those regions in which mammographic screening programmes were fully implemented the most rapidly. Although a very slight decline in breast cancer incidence was noted in Denmark between 2003 and 2007 (−0.4% annual percentage change), that was not statistically significant.41 Peak HRT use was less than 12% in 2002, and the absolute decrease in use by 2008 was only 3%.
Countries with a time lag between declining HRT use and breast cancer incidence
As described earlier, a decrease in breast cancer incidence occurred very soon after HRT use began to decline in many Western nations. However, in several countries, a time lag between these trends has been observed. In many instances the magnitude of the decline in breast cancer incidence is significantly smaller than that in the USA and other nations with no time lag.
Scotland
Initial reports from Scotland suggested no decline in breast cancer incidence after 2002 despite a decline in HRT use. Peak HRT use was 20% in 2000, followed by a 62% decline by 2007.46 However, a modest decline in breast cancer incidence in women aged 50–64 years between 2000 and 2005 has subsequently been described.47 However, the relatively modest 11% decrease in breast cancer incidence over the 5 year period did not reach statistical significance until 2005.48 The authors suggest the modest decline in breast cancer incidence in Scotland compared to the USA reflected lower peak HRT use. Additionally, the extension of mammographic screening to women aged 65–70 years during this period appeared to be a significant confounding factor when examining trends in women over 50 years as a whole.48
Norway
An initial report from Norway suggested no decline in breast cancer incidence after 2002 despite reductions in HRT use similar to those seen in the USA.49 Peak usage of HRT by 2000 was 35–40% and decreased nearly 50% between 2002 and 2006. The initial publication utilised data from four counties in Norway that represented only 25% of the Norwegian population. Updated data from the national Norwegian cancer registry, encompassing the vast majority of the country, did show a modest decline in breast cancer incidence in women aged 50–69 years, beginning in 2004 and continuing to 2006 (the authors did not quantify the decrease).37 National screening mammography programmes continued to expand until 2004 in many regions. It has been suggested that one reason for the discordant findings of the two Norwegian studies is the varying uptake of screening mammography between the different regions of Norway at the time of analysis.50
Sweden
An initial report from Sweden suggested no decrease in breast cancer incidence after 2002, despite reductions in HRT use similar to the USA.49 However, a recent publication has suggested that a decline did occur in women aged 50–59 years, in whom HRT use was highest.50 In this age group HRT use peaked in 1999 at 36%, and decreased to 27% by 2002 and subsequently to 9% by 2007. A significant decline in breast cancer incidence between 2003 and 2007 of 4.5% per year was evident in women aged 50–59 years, but not in younger or older women. Thus there appeared to be a time lag of 4–5 years from the initial decline in HRT use and a decrease in breast cancer incidence. Screening mammography coverage for this region was complete by 1997, and therefore rates of screening were likely stable during this period. A less abrupt decline in HRT use compared to other countries may potentially account for the time lag evident in Sweden.
Trends in populations of non-European ancestry
Utilising SEER data, changes in breast cancer incidence in women of Hispanic, Asian and African-American ancestry were compared to non-Hispanic whites (NHWs).51 Compared to NHWs, the decline in breast cancer incidence was attenuated (and not statistically significant) in Asians and Hispanics; no decline was evident in African-Americans. HRT use varied considerably among ethnicities, being most prevalent in NHWs and progressively lower in Asians, Hispanics and African-Americans.52 The authors concluded that the lack of a decline in breast cancer incidence in African-Americans reflects the lower peak prevalence of HRT use. Additionally, there is some suggestion that the magnitude of HRT discontinuation post-WHI was smaller in African-Americans compared to Caucasians.51 Finally, African-Americans have higher rates of hormone receptor negative cancers, suggesting that inherent differences in tumour biology among different ethnicities may also play a role.53 Similar results have been described by Krieger et al, who additionally reported that the decline in breast cancer was limited to women living in high income counties.54
Given the very low prevalence of HRT in countries such as China (figure 2) and much of the developing world, it is unlikely that changes in HRT use have had a sizeable impact on breast cancer incidence in these regions. For example, in Thailand and Japan, HRT use was only 5–6% (ever users); not surprisingly, no association between HRT use and breast cancer incidence was evident in either country.55 56
A decline in breast cancer incidence prior to 2002?
Several reports from the USA have suggested that there was a decline in breast cancer incidence in 1999 or 2000, at least 2 years prior to the initial WHI publications.54 57 58 Explanations for this decline include the mammographic detection of pre-invasive carcinoma in situ (thereby preventing invasive breast cancers), saturation of mammographic screening and declining mammography rates. Additionally, HRT use in the USA actually peaked in 1999, and thereafter began to decline, albeit less rapidly than the decline seen after 2002.54 One potential explanation for this decrease in HRT use was knowledge of the HERS trial, published in 1998, which failed to demonstrate a protective effect of HRT on the secondary prevention of coronary artery disease.59
Irrespective of the aetiology, this earlier decline in breast cancer incidence is modest compared to the decline after 2002.57 Similar declines predating 2002 have been described in Germany.34 A modest decline in breast cancer incidence beginning in 2000 has also been described in Canada. However, the decline was statistically significant only in women over 75 years of age.21 Given the lower prevalence of HRT use in this age group, it seems unlikely that cessation of HRT use was a major factor influencing this decline. In the UK, HRT use peaked at 25% in 2000 and thereafter began to decline, with a more precipitous decrease after 2002.60 Breast cancer incidence declined a modest 0.8% per year from 1999 to 2006 in women 50–59 years of age. It is possible that the addition of two-view mammograms (which increase sensitivity) to the national screening programme in 2001 significantly confounded the trend between HRT use and breast cancer incidence in the UK during this time period.
Conclusions
Publications of the WHI trials lead to a precipitous decline in HRT use in many countries. Subsequently, many of these same countries experienced a decline in breast cancer incidence. However, the timeline and magnitude of the decline in breast cancer incidence show significant variability. The reduction in breast cancer incidence was most pronounced in countries where peak prevalence of HRT use was quite high. Conversely, countries with lower HRT use showed more modest (or absent) declines in breast cancer incidence, often occurring several years after HRT use began to decline. In some instances, the decline in breast cancer incidence in such countries was more likely the result of changes in mammography rates or saturation of mammographic screening programmes rather than changes in HRT use. Thus, the absolute decline in HRT use for a country or region appears to be an important determinant of the magnitude of the decline in breast cancer incidence. For much of the non-Western world, peak HRT use was historically very low, and as such, minimal influence of HRT use on breast cancer incidence is anticipated.
For many countries, it is difficult to disentangle changes in mammographic screening rates from changes in HRT use when examining trends in breast cancer incidence. Additionally, gene–environment interactions and demographic factors known to influence breast cancer risk (such as age at menarche and childbearing) could potentially modify the influence of HRT trends on breast cancer incidence. However, the relative importance of these factors is unclear at this time. One study based on statistical modelling suggests that in the USA, hormone use was unlikely to account for more than half of the observed decline in breast cancer incidence between 2002 and 2003.61
Although there may be significant variability in magnitude and timing, the evidence is compelling that HRT use increases the risk of breast cancer, and its cessation reduces this risk. As an illustration, the available evidence readily fulfils the majority of the Bradford–Hill criteria for establishing causation (table 4). Whether the observed decline in breast cancer incidence will be sustained (preliminary data from the USA suggests it might not be),64 and whether breast cancer mortality will also decline, are important questions that currently remain unanswered.
The Bradford–Hill criteria for assessing causation, applied to the association between decreasing hormone replacement therapy (HRT) use and declining breast cancer incidence
Acknowledgments
SSA holds the Michael G. DeGroote Heart and Stroke Foundation of Ontario Chair in Population Health and the May Cohen Eli Lilly Endowed Chair in Women's Health Research, McMaster University.
References
Footnotes
Provenance and peer review Commissioned; externally peer reviewed.