Article Text

Abstract
Objectives: To evaluate the microbiological cure rate after treatment with tetracyclines or azithromycin in patients infected with M genitalium.
Methods: One hundred and fifty-two men and 60 women positive for M genitalium were recruited. Patients treated either with doxycyline for 9 days or with azithromycin 1 g stat. were compared. Those still positive for M genitalium after primary doxycycline treatment received an extended course of azithromycin 500 mg on day 1 followed by 250 mg daily for the following 4 days, whereas those with treatment failure after azithromycin received doxycycline 100 mg twice daily for 15 days.
Results: The eradication rate after azithromycin 1 g stat. was 85% (95% CI 69 to 94) in men (n = 39) and 88% (95% CI 64 to 99) in women (n = 17) and after doxycycline 17% (95% CI 9 to 27) in men (n = 76) and 37% (95% CI 19 to 58) in women (n = 27). Extended azithromycin eradicated M genitalium from 96% (95% CI 85 to 99) of the men (n = 47) and from all six women who failed on doxycycline. Extended doxycycline treatment was insufficient. Persistent urethral inflammation was seen in a substantial portion of the men after eradication of M genitalium regardless of the antibiotic drug, indicating a poor predictive value of urethral smears in evaluation of persistent or recurrent infection.
Conclusions: Azithromycin was more effective than doxycycline in treating patients infected with M genitalium. The extended course of azithromycin was highly effective but was given after the initial treatment with doxycycline. Randomised clinical trials are needed to compare the different dosages of azithromycin.
Statistics from Altmetric.com
Mycoplasma genitalium was first isolated in 1980 from male patients with urethritis.1 The bacterium is very difficult to isolate by culture, but specific PCR-methods have made it possible to detect M genitalium.2 3 The clinical picture of a M genitalium infection resembles that of a Chlamydia trachomatis infection. The two bacteria are relatively rarely found together, indicating that they may act as separate causes of disease. There is accumulating evidence that M genitalium causes urethritis in men, and urethritis and cervicitis in women, and that it is sexually transmitted.4–11 Further studies are needed to evaluate the role of M genitalium in upper genital infections and late sequelae such as infertility.12 Like other mycoplasmas, M genitalium lacks a cell wall, and thus is inherently resistant to beta-lactam antibiotics and other cell wall inhibitors. It adheres to epithelial cell membranes and has been reported to grow and replicate intracellularly in vitro.13 14 In general, mycoplasmas are susceptible to antibiotics that inhibit protein synthesis, and most of these antibiotics have a bacteriostatic effect. In in vitro studies, M genitalium is reported to be susceptible to tetracyclines and macrolides (including newer macrolides called ketolides), and highly susceptible to azithromycin and some of the newer quinolones.15–18 Most of these data originate from a few laboratory strains of M genitalium, and only recently have a larger number of strains been examined.19 It was shown that several strains could be considered resistant to tetracyclines and to some of the older fluoroquinolones.
In Scandinavia, the majority of sexually transmitted infection (STI) clinics use doxycycline and/or azithromycin as the primary treatment for non-gonococcal urethritis (NGU) and cervicitis. Only one controlled clinical trial concerning treatment of M genitalium has been presented, showing that azithromycin given as 1 g stat. is more effective than doxycycline 100 mg twice daily for 7 days.20 Azithromycin eradicated M genitalium from 84% of the patients, but treatment failure in as many as 28% has been reported from Australia.21 Most of the patients harbouring M genitalium after antibiotic treatment experience symptoms of persistent or recurrent urethritis.22–24
The main purpose of the present study was to evaluate the outcome of standard treatments given to STI-clinic attendees with signs and symptoms of non-gonococcal urethritis and cervicitis and subsequently found positive for M genitalium. The study was approved by the Medical Products Agency in Sweden and by the Regional Ethical Review Boards and was performed independent of the pharmaceutical industry.
METHODS
Patients aged 18 years or older were recruited at six different STI clinics in Norway and Sweden between January 2002 and May 2004. Apart from routine screening tests for C trachomatis, N gonorrhoeae, HIV and syphilis, patients, primarily those with symptoms of urethritis and/or cervicitis, were offered a test for M genitalium. Patients with symptomatic partners were also tested. The patients were treated with antibiotics according to the standard procedure, that is doxycycline 200 mg day 1 and 100 mg days 2–9 or azithromycin 1 g as a single dose (stat.). The treatment was initiated at the first visit before any test results were known. At the follow-up visit and after informed consent, those patients positive for M genitalium and negative in the routine screening tests at the initial visit were included in the study.
Patients still positive for M genitalium at follow-up were treated with azithromycin 500 mg on day 1 and 250 mg on days 2–5 if a tetracycline was given initially and with doxycycline 100 mg twice daily for 15 days if azithromycin was given initially (extended treatment). In order to be eligible for evaluation of the different treatments, the follow-up visits were to take place 20–56 days after initiation of treatment. An evaluation of the response rate was also performed comparing early follow-up (20–30 days) with late follow-up (31–56 days). Each patient was told to abstain from sexual intercourse during treatment and until the present sexual partner had been treated.
A medical history review and a clinical examination were performed at each visit according to a standardised protocol. Urethral and cervical smears were taken, stained in Methylene Blue and examined at 1000× magnification for the presence of polymorphonuclear leucocytes (PMNLs). Vaginal wet smears were examined for the presence of PMNLs, clue cells, Trichomonas vaginalis and yeasts. Urethritis was defined as ⩾5 PMNLs in urethral smears. Cervicitis was diagnosed when ⩾30 PMNLs were seen in cervical smears and more PMNLs than epithelial cells were observed in the wet smear. The symptoms considered were dysuria, urethral itch, discharge from the urethra and/or vagina and bleeding abnormalities. Nucleic acid amplification tests (NAATs) for C trachomatis and cultures for N gonorrhoeae were carried out according to the routines of each clinic. First, void urine and cervical specimens were sent by mail to Statens Serum Institut in Copenhagen, Denmark for detection of M genitalium by PCR as previously described.25 One centre (Falun in Sweden) analysed the specimens in the local laboratory using minor modifications of the same method.26
Fisher’s exact test (two-tailed) was used to test for differences in proportions, and the proportion difference with 95% confidence interval is given. The Mann–Whitney test was used to test differences in continuous variables between groups.
RESULTS
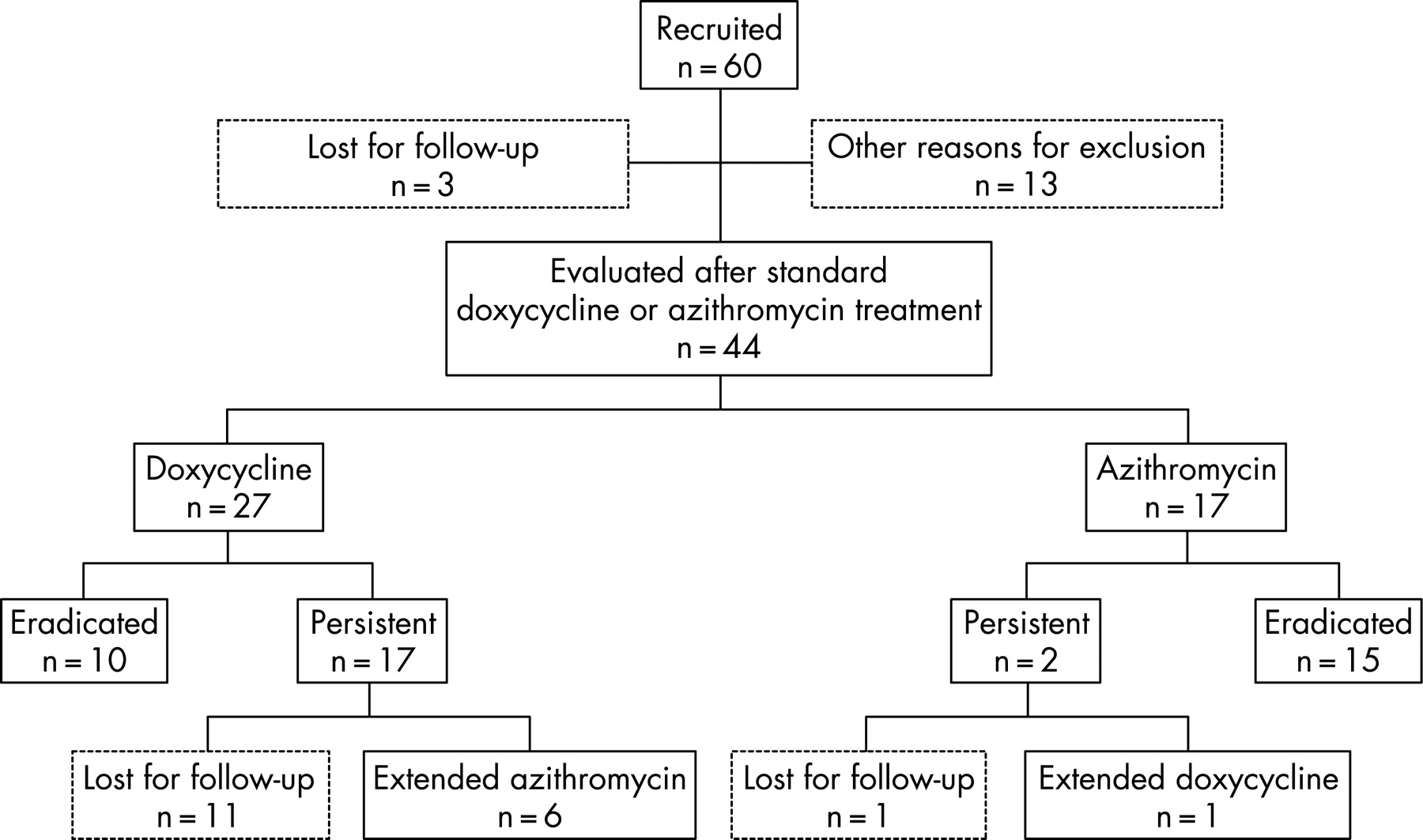
Two hundred and twelve patients were recruited, and 159 were eligible for evaluation of the effect of doxycycline versus azithromycin standard treatment. Fifty-three patients were excluded; 18 were lost for follow-up, seven patients received lymecycline as standard treatment, and 28 had wrong inclusion criteria such as recent antibiotic treatment or were not followed up within the scheduled time frame. Fifty-seven patients who failed the initial treatment were available for evaluation after extended treatment with azithromycin and doxycycline (figs 1 and 2).


{kind=link}
{kind=link}
One clinic used only azithromycin and one only doxycycline, whereas four clinics used primarily doxycycline but switched to azithromycin for initial treatment during the study period.
The median age of the recruited patients was 27 years (range 18–61 years) for men and 24 years (range 19–42 years) for women. There was no difference in age between the treatment groups (p = 0.67 for men and p = 0.95 for women). All patients, except two men, reported heterosexual contacts only.
Initial treatment
Men (table 1)
Of the 76 men initially treated with doxycycline, 13 (17% (95% CI: 9 to 27)) had a negative M genitalium PCR test at the follow-up visit. The eradication rate was 12% (5/43) and 24% (8/33) for early and late follow-up respectively (p = 0.219; proportion difference −0.13 (−0.31 to 0.05)).
Of the 39 men initially treated with azithromycin 1 g stat., 33 (85% (95% CI: 69 to 94)) had a negative M genitalium PCR test at the follow-up visit. There was no difference between early (18/22 82%) and late (15/17 88%) follow-up (proportion difference 0.06 (−0.20 to 0.30)). The microbiological cure rate was significantly better (p<0.001) for azithromycin 1 g stat. than for doxycycline.
There were no differences between early and late follow-up regarding the effect on signs and symptoms. Despite eradication of M genitalium, a considerable number of men still had positive smears (6/13 after doxycycline and 15/31 after azithromycin; proportion difference 0.02 (−0.32 to 0.29)) and reported clinical symptoms (4/11 after doxycycline and 4/25 after azithromycin; proportion difference 0.20 (−0.09 to 0.52)).
Women (table 2)
Of the 27 women initially treated with doxycycline, 10 (37% (95% CI: 19 to 58)) had a negative M genitalium PCR test at the follow-up visit. The eradication rate was 30% (3/10) and 41% (7/17) for early and late follow-up respectively (p = 0.692; proportion difference 0.11 (−0.44 to 0.27)). Of the 17 women initially treated with azithromycin, 15 (88% (95% CI: 64 to 99)) had a negative M genitalium PCR test at the follow-up visit. The eradication rate was 80% (4/5) and 92% (11/12) for early and late follow-up, respectively (p = 0.515; proportion difference −0.12 (−0.57 to 0.23)). Azithromycin was significantly more efficient in eradicating M genitalium than was doxycycline (p = 0.0014).
Due to inconsistent sampling at the initial visit, only a few women could be evaluated regarding signs and symptoms. There were still some women who did not respond clinically, although M genitalium was eradicated.
Extended treatment
Men (table 3)
The extended azithromycin treatment was evaluated in 47 men who failed the initial doxycycline treatment. The microbiological eradication rate was 96% (95% CI: 85 to 99). Due to the low number of patients failing initial therapy with azithromycin, only three men were given the extended doxycycline treatment, and two had a negative M genitalium PCR at follow-up. Notably, none of the three men with clinical symptoms became asymptomatic.
Women
All six women, receiving extended azithromycin treatment after initial doxycycline failure, had negative M genitalium PCR tests at the follow-up visit (100% (95% CI: 54 to100)).
The single woman receiving extended doxycycline treatment failed to respond both microbiologically and clinically.
Azithromycin 1 g stat. versus azithromycin extended treatment
For all comparisons between extended azithromycin and 1 g stat., it should be noted that the two groups are not directly comparable, as the patients treated with extended azithromycin had failed on initial doxycycline treatment.
The response rate was better for the extended treatment (45/47 96%) than for the initial (33/39 85%), but this did not reach statistical significance (p = 0.133; proportion difference 0.11 (−0.01 to 0.26)).
Treatment effects in men versus women
There was no gender difference in the microbiological eradication rate after azithromycin 1 g stat. or after extended azithromycin treatment. For both men and women, the eradication rate as well as the clinical response after doxycycline treatment was poor. However, women appeared to achieve higher eradication rates than did men, as 10/27 (37%) of the women cleared the infection as compared with 13/76 (17%) of the men (p = 0.057; proportion difference 0.20 (0.01 to 0.40)). The number of patients receiving the extended doxycycline treatment was too small to permit conclusions.
DISCUSSION
We found that the azithromycin treatment was significantly better than the doxycycline treatment. The microbiological response rate of azithromycin 1 g was relatively high in both males (85%) and females (88%), but a treatment efficacy lower than 95% is generally not considered acceptable in treatment of STIs. The extended treatment with azithromycin seemed to be more effective than single-dose treatment, since 96% and 100% of men and women, respectively, had M genitalium eradicated.
This study was initiated when little was known about the effect of antibiotics on M genitalium infections. As a result of the study, the extended treatment with azithromycin is now the recommended treatment of M genitalium infections in Scandinavia. We are aware that the study design was an open treatment trial. However, since the main outcome measure was eradication of M genitalium, this should not change the conclusions. Furthermore, the low number of patients in some of the groups may limit our conclusions.
Two earlier studies have found that tetracyclines have a good treatment efficacy.5 8 However, several other reports have described persistence of M genitalium and recurrence of symptoms after tetracyclines27 and a much better effect of azithromycin treatment in eradicating M genitalium.28 In a recent randomised clinical trial performed in the US comparing azithromycin 1 g stat. to doxycycline 100 mg twice daily for 7 days in men with urethritis, eradication rates were found to be very comparable with those found in the present study with an eradication rate of 84% after azithromycin compared with only 36% after doxycycline.20 Differences in dosage schemes and the timing of follow-up specimens can at least partly explain the differences between studies regarding the efficacy of tetracyclines, but local differences in the susceptibility pattern may also play a role.
Although the overall response to doxycycline was very poor, females had a higher microbiological eradication rate than did males, 37% versus 17%. The reason for this discrepancy is unclear. It might be speculated that men harbour M genitalium in compartments (eg, the prostate gland) that are not reached by sufficiently high concentrations of doxycycline to eradicate the bacteria.
There was a trend towards a higher microbiological cure rate in patients attending for late follow-up than for those attending early. This may indicate that non-viable M genitalium DNA is still present if the test of cure is made early, that is before 31 days, or it may reflect that patients with persisting symptoms re-attended earlier. With a late follow-up, it can be questioned whether a positive PCR test for M genitalium indicates an unsuccessful treatment or a re-infection. Our patients were urged to abstain from sexual activities until follow-up and questioned about adherence to this, but no difference was observed between the different treatment groups. This should exclude re-infection as a cause of the different efficacy of doxycycline and azithromycin.
The observed clinical outcome of treatment with doxycycline, regarding signs and symptoms in both men and women, was similar to that observed after azithromycin 1 g stat. when only patients with successful eradication of M genitalium were considered. A surprising finding was that although the initial azithromycin treatment with 1 g had a high microbiological cure rate, signs of persistent inflammation were seen in 15/31 (48%) of the M genitalium negative men at follow-up. This is in the same range as that after a microbiologically successful doxycycline treatment with 6/13 (46%) of the men having persistent signs. Thus, a urethral smear appears to be a poor predictor of microbiological response to treatment. The proportion of men who experienced relief of symptoms was 84% after azithromycin treatment, which is more in line with the microbiological eradication rate. Another unexpected finding was that among the women with clinical signs and symptoms at inclusion clearing the infection, only half of them responded clinically in both of the azithromycin treatment groups. This may indicate that a longer follow-up period is necessary for evaluation of the clinical response.
In most clinical settings, treatment is given before the test results are known, and in many clinics the patient will receive doxycycline. Non-responders who are Chlamydia-negative should be offered a test for M genitalium, and if positive, our results indicate that the 5-day treatment with azithromycin will cure most patients, whereas the 1 g stat. is insufficient in an unacceptable proportion of the patients. It can also be speculated that a suboptimal dose of azithromycin may increase the risk of resistance development.21 It should be noted that no large studies have been published that suggest the use of extended azithromycin treatment in NGU and cervicitis in general. However, it has been shown that dividing 1 g of azithromycin into 500 mg day 1 and 250 mg on days 2 and 3 was significantly better than 1 g azithromycin stat. or doxycycline 200 mg for 7 days in reducing symptoms and clearance of signs of urethritis.29 Although that study did not include detection of M genitalium, it does encourage larger randomised trials to establish both the best treatment of patients infected with M genitalium as well as NGU in general.
Key messages
This study indicates that azithromycin 500 mg on day 1 and 250 mg on days 2–5 can be considered as the first line treatment of M genitalium in men and women
Doxycycline is not appropriate for treatment of M genitalium
A urethral smear appears to be a poor predictor of microbiological response to treatment
Acknowledgments
Gun-Britt Karlberg, Department of Dermatovenereology, Karolinska University Hospital, Huddinge, Sweden is thanked for excellent support in monitoring the study. Birthe Dohn, Statens Serum Institut, Copenhagen, Denmark, and Britta Loré, Central Hospital, Falun, Sweden are thanked for excellent technical assistance.
REFERENCES
Footnotes
Parts of this study were presented at the 15th Meeting of the International Society for Sexually Transmitted Diseases Research, Ottawa, Canada, July 2003.
EB was the principal investigator for the study. All authors contributed to the study design. EB, CA, GB, HC, GJ, EJ, HM and PL collected the clinical data. JSJ performed most of the PCR analyses. EB, PL and JSJ prepared the manuscript, which was reviewed by all authors.
Funding: The study was supported by grants from the Edvard Welander and Finsen Foundations.
Competing interests: None.