Article Text

Abstract
Objectives: The enhanced sensitivity of nucleic acid amplification tests (NAAT) provides an opportunity for estimating the prevalence of untreated Chlamydia trachomatis infections. The transmissibility and public health significance of some NAAT-identified infections are, however, not known.
Methods: Adults attending an urban emergency department provided specimens for C trachomatis screening using NAAT. Participants testing positive were offered follow-up including re-testing for C trachomatis using NAAT and traditional methods, eg culture and direct fluorescent antibody, and were treated. Partners were offered identical evaluation and treatment. Overall, 90 C trachomatis-positive participants had one or more sexual partners enrolled.
Results: Evidence of transmission, as defined by infection concordance between partnerships, was observed among 75% of partners of index cases testing positive by both NAAT and traditional assay but only 45% of partners of index cases testing positive by NAAT only (prevalence ratio 1.7, 95% CI 1.1 to 2.5). Among index participants returning for follow-up, 17% had no evidence of C trachomatis infection by NAAT or traditional assay (median follow-up three weeks).
Conclusions: A substantial proportion of positive NAAT results for chlamydial infection may be of lower transmissibility and may not persist after a short follow-up. The long-term health effects of some positive NAAT are uncertain.
Statistics from Altmetric.com
Unrecognised Chlamydia trachomatis infection is common among US young adults.1–3 Estimates of the prevalence of C trachomatis have been facilitated by the development of non-invasive nucleic acid amplification tests (NAAT). NAAT provide substantial improvements in test sensitivity while retaining the high specificity of traditional methods.4 The use of NAAT, compared with culture, increases the yield of infections detected by 20–40%.5
Although the enhanced sensitivity of NAAT is well recognised, the significance and transmissibility of the additional infections detected by NAAT are unknown. It is possible that NAAT is detecting clinically inconsequential infections involving low levels of viable organisms, or perhaps amplifiable residual DNA from a recently controlled infection.
We conducted a cross-sectional study with recruitment of sexual partners to examine the potential transmissibility of chlamydial infections identified by NAAT but not by traditional assay. We tested the hypothesis that chlamydial infections that are detectable only by NAAT are less transmissible, as evidenced by infection concordance within partnerships, than infections that are also detectable by traditional methods. As a secondary aim, we examined the persistence of NAAT-positive infections among participants after a short follow-up.
METHODS
Between November 2002 and February 2005, trained interviewers approached adult patients attending the Johns Hopkins Hospital Emergency Department to assess eligibility for C trachomatis screening, eg age between 18 and 35 years, English speaking, and sexually active in the past 90 days. Eligible adults who consented to screening also completed a brief audio computer-assisted self interview about recent sexual and health behaviours.6 Participants screened in the emergency department after March 2003 received a US$10 food coupon.
We obtained contact information from all index participants undergoing C trachomatis screening in the emergency department to facilitate the follow-up of positive test results by trained research disease intervention specialists. Disease intervention specialists offered follow-up examination to detect clinical evidence consistent with chlamydial infection, additional C trachomatis testing (NAAT and traditional assay), and treatment at the Johns Hopkins Hospital General Clinical Research Center (GCRC). Disease intervention specialists also contacted up to five named sexual partners within the past 60 days and offered evaluation and treatment procedures identical to those provided to index participants. Index participants and partners presenting to the GCRC for follow-up completed a detailed behavioural audio computer-assisted self interview and received US$50–200 in compensation for their time and travel costs. Partners not attending the GCRC were offered the option of a home visit to complete the questionnaire and to collect a specimen for NAAT.
The Research Triangle Institute, University of North Carolina, and Western (for the Johns Hopkins University School of Medicine) Institutional Review Boards approved all study procedures. Study participants with positive test results for chlamydial infection were reported to the Baltimore City Health Department.
Specimen collection and laboratory testing
NAAT for C trachomatis
US Food and Drug Administration-approved NAAT were performed according to the manufacturers’ instructions at the University of North Carolina. Initially, urine specimens were tested using a ligase chain reaction (LCR) assay (Abbott Laboratories, North Chicago, Illinois, USA). After the LCR was withdrawn from the market in 2003, male urine specimens and female vaginal swabs were tested using the COBAS Amplicor PCR assay (Roche Diagnostic Systems, Indianapolis, Indiana, USA).7 8 Positive NAAT results were confirmed by repeating the assay. Infection with C trachomatis as detected by NAAT (N+) was defined as a repeatedly positive test on the same specimen.
At follow-up, NAAT were performed on urine (men throughout the study and women initially), urethral swabs (men), endocervical swabs (women), and self-administered vaginal swabs. Each index thus received three NAAT: one upon initial recruitment in the emergency department and two repeat tests on follow-up. Sexual partners received two NAAT during their GCRC visit.
Traditional assay for C trachomatis
Traditional testing was performed at GCRC follow-up using culture and direct fluorescent antibody (DFA) from urethral and endocervical specimens. Specimens were stored at −80°C until testing by the International STD Research Laboratory, Johns Hopkins University. Culture was performed in McCoy cells. Culture-negative specimens were tested using DFA of the sediment from the centrifuged culture transport media; a slide was considered DFA positive if three or more elementary bodies were present. Culture-positive specimens and DFA-positive/culture-negative specimens were considered positive for C trachomatis by traditional assay (T+). Specimens that tested culture and DFA negative were considered traditional assay negative (T−).
Statistical analyses and outcomes
Chi-square and t-tests were used to compare characteristics of NAAT-positive index participants who did and did not present for follow-up.
We assessed the concordance of infection between sexual partners as a surrogate for the transmissibility of NAAT-identified infections, restricted to partnerships in which both NAAT and traditional test results were available. We defined concordance as either a positive NAAT (N+) or traditional assay (T+) result for C trachomatis among partners of C trachomatis-positive index participants. All index participants were considered NAAT positive on the basis of their emergency department test result.
Our primary hypothesis was that chlamydial infections detectable by NAAT but not by traditional assay (N+T−) in the index participants would be less transmissible to sexual partners than infections that were also detectable by traditional assay (N+T+). Non-concordance was considered as evidence of lower transmissibility. We tested this hypothesis by examining prevalence ratios with 95% CI that compared the proportion of partnerships with concordant C trachomatis infections (N+ and/or T+) between index participants who tested N+T− and those who tested N+T+.
We also examined characteristics of index participants and their partners that may be associated with infection concordance. For all partnership analyses, we used generalised estimating equations with a log link and binomial error distribution to estimate prevalence ratios for concordance. Generalised estimating equations account for within-group correlation, such as that that exists between multiple partners of the same index participant.9
As a secondary aim, we examined the persistence of NAAT-identified chlamydial infections at follow-up among individuals with positive NAAT in the emergency department. Factors potentially influencing persistence were examined in binomial regression analyses. In addition, we examined the association between the persistence and concordance of infection within partnerships. All statistical analyses were conducted using Stata version 8 (Stata Corp., College Station, Texas, USA).
RESULTS
Study recruitment: C trachomatis screening and follow-up
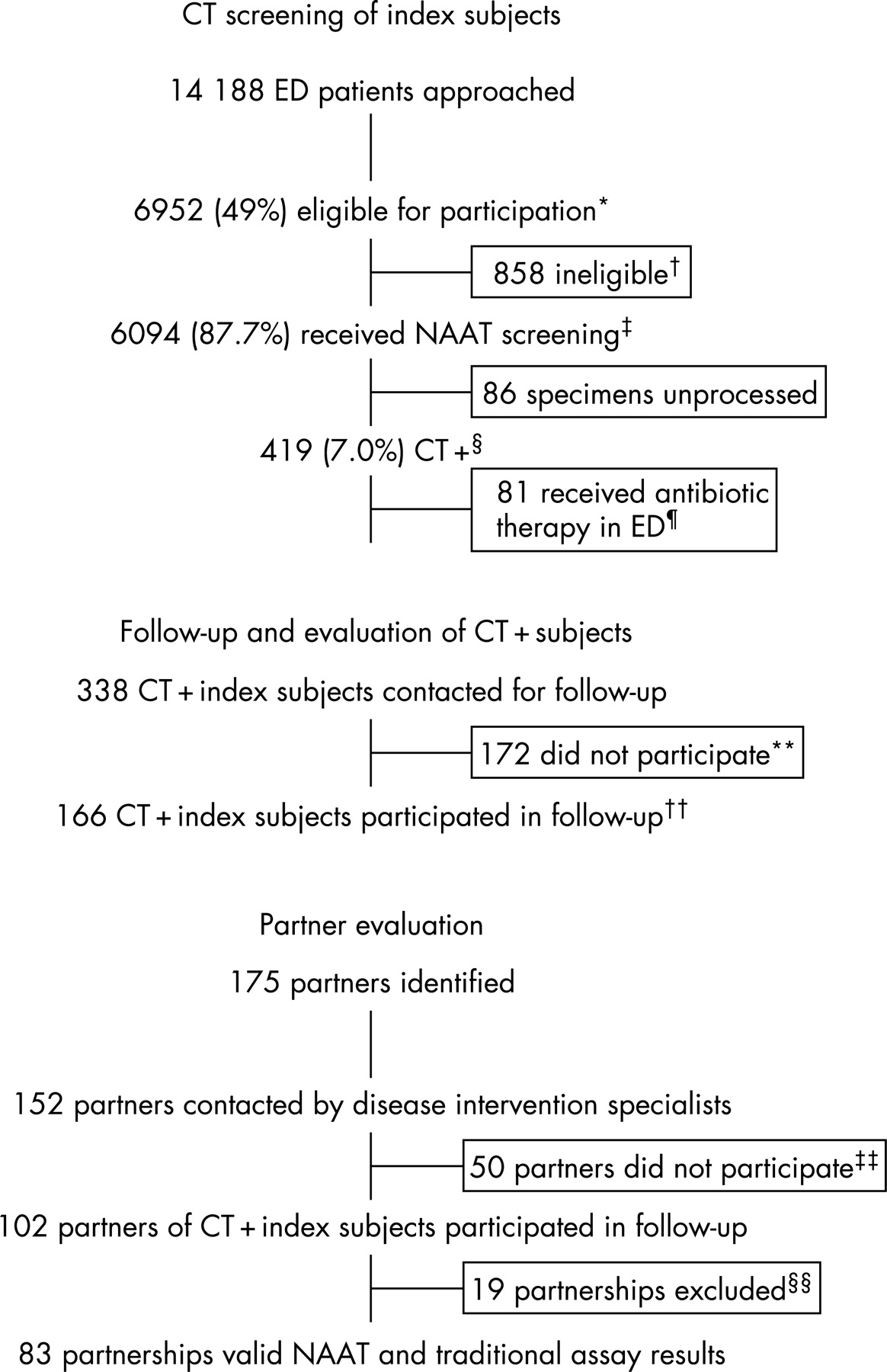
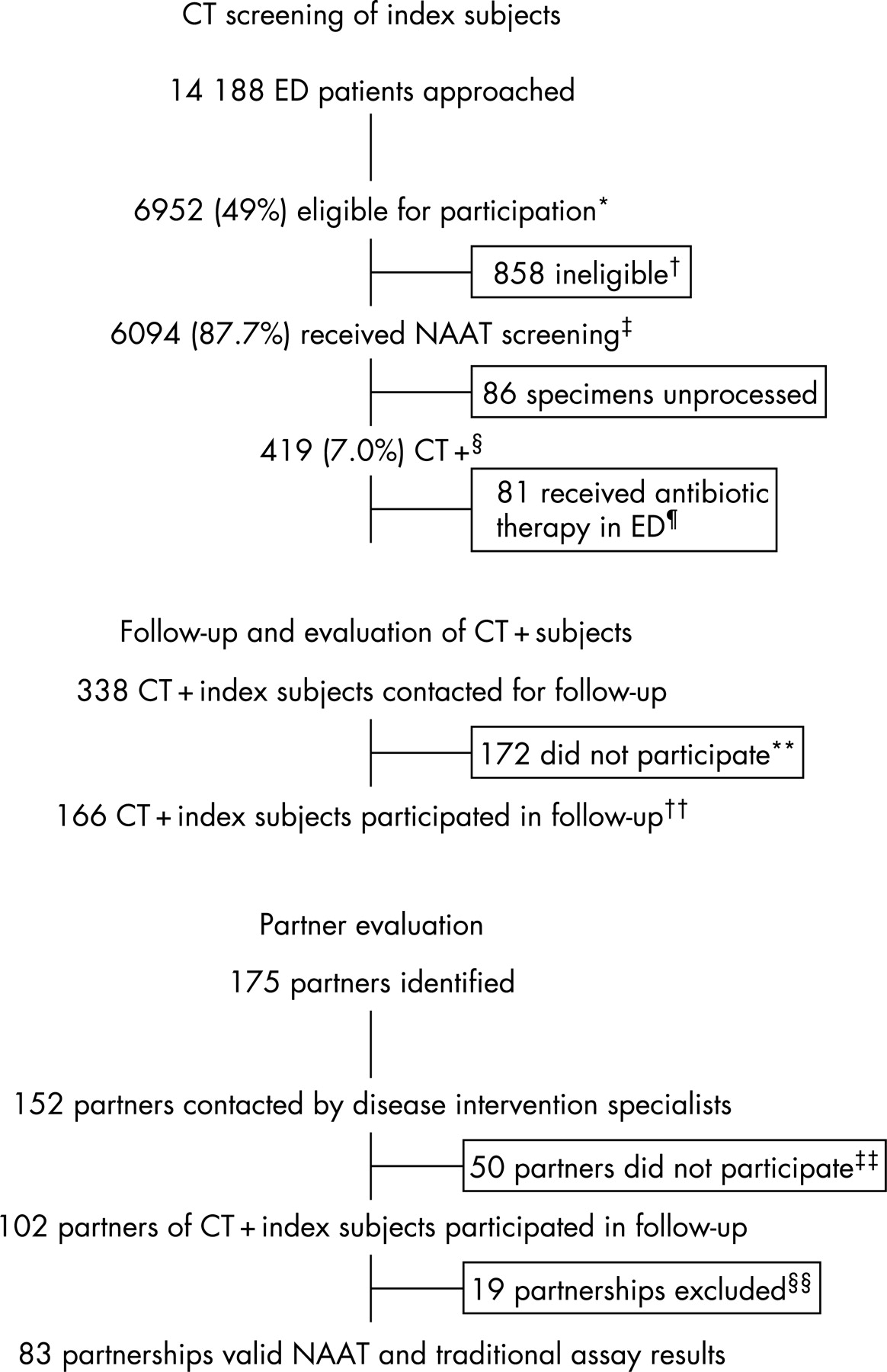
Over a 27-month period, 21 trained interviewers identified 6952 eligible adults attending the emergency department (fig 1); 6094 (87.7%) consented to screening. The prevalence of chlamydial infection was 7.0% in emergency department participants. The prevalence of C trachomatis in male urine specimens (7%) was comparable as determined by LCR and PCR (8.4% versus 6.6%, p>0.10). Among female urine specimens tested by LCR (November 2002 to August 2003), 6.8% were C trachomatis positive; 7.3% of female swab specimens tested positive by PCR (p>0.10).
{kind=link}
Of the 419 index participants who tested NAAT positive, 81 (19.3%) received antibiotic treatment during their emergency department visit. Of the remaining 338, 166 (49%) participated in follow-up. The mean number of disease intervention specialist contacts was two (range one to 10) and the average number of days between emergency department testing and follow-up was 21.5 (range eight to 46 days). Participants at follow-up were slightly younger (mean age 22.5 versus 23.5 years; p = 0.04) and more were women (62% versus 50.6%, p = 0.03) compared with those who did not participate (table 1).
Most index participants (87%) named one or more recent sexual partners at follow-up; 13% refused to provide partner information. Of 175 partners identified, 152 (86.9%) were contacted successfully by disease intervention specialists and 102 (58.3%) attended follow-up. Nearly half (48%) of the partnerships presented for follow-up together.
Partner concordance of C trachomatis infections
Our concordance analyses are limited to the 83 heterosexual couples (72 index participants with one partner, four indexes with two partners, and one index with three partners) for whom both NAAT and traditional assay results were available. We excluded 17 partnerships because of missing results, inadequate specimen collection, transcription error, or multiple enrollment of a positive index subject. Two exclusively male partnerships were omitted as we did not collect anal or throat specimens.
Evidence of infection transmission, as defined by concordance within partnerships, was more common among index cases testing positive by both NAAT and traditional assay (N+T+) than among index cases testing positive by NAAT alone (N+T−; table 2). Evidence of transmission was observed in 39 of 52 partners (75%) of N+T+ index cases, but only 14 of 31 partners (45%) of N+T− index cases (prevalence ratio 1.7, 95% CI 1.1 to 2.5).
The relationship between index test result (N+T− or N+T+) and partner concordance did not vary by gender. Among the male partners of N+T+ female indexes, 82% were concordant for C trachomatis, compared with 46% of male partners of N+T− women. Similarly, 70% of female partners of N+T+ index men were concordant, in comparison with 43% of female partners of men testing positive by NAAT only. There was no difference by index’s or partner’s age, the number of new partners in the past three months, a history of chlamydial infection, a history of any sexually transmitted infection, antibiotic use before the follow-up visit, or time to index follow-up. Adjusting for the timing of the partner visit, however, reduced the prevalence ratio to 1.5 (95% CI 1.03 to 2.2). Partners presenting at the same time as the index participant were more likely to test concordant than partners presenting after the index visit.
Limiting traditional test results to culture only decreased our overall estimate of concordance from 64% to 54% (prevalence ratio 1.4, 95% CI 0.93 to 2.0). Differences in the type of NAAT (LCR versus PCR) or specimen type (female urine versus vaginal swab) could also influence our transmission estimates. Although all women screened in the emergency department provided vaginal swabs for C trachomatis testing using PCR, initially women also provided urine specimens for LCR testing. When the LCR was withdrawn in 2003, male urine samples and female swabs were tested using PCR. Restricting our concordance analysis to include only female indexes with positive swab results (n = 81 couples, prevalence ratio 1.7, 95% CI 1.1 to 2.5) or male and female index subjects with positive PCR results alone (n = 75 couples, prevalence ratio 1.7, 95% CI 1.2 to 2.5) had no effect on our transmission estimates.
Non-persistence of NAAT-positive results
Index participants were screened initially in the emergency department and re-evaluated at follow-up, thus it is possible to examine the short-term persistence of NAAT-identified C trachomatis. Among participants who had not received antibiotic therapy during the emergency department visit and who had both NAAT and traditional assay results available for follow-up (n = 163; three participants had missing traditional assay results), 27 (17%) individuals had no evidence of C trachomatis infection by NAAT or culture/DFA. Nine (5%) individuals were NAAT negative, but positive by culture/DFA. The remaining 127 (78%) participants were NAAT positive (table 3).
In bivariable analyses, women were significantly more likely than men to test negative for C trachomatis after a short follow-up (23% versus 6%, risk ratio 3.6, 95% CI 1.3 to 9.9) as were individuals who had used antibiotics in the three months before their emergency department visit (32% versus 12%, risk ratio 2.6, 95% CI 1.2 to 5.5). In multivariable analyses, only gender remained significantly associated with the persistence of NAAT-positive results.
Non-persistence and partner concordance
We also examined the association between the persistence of NAAT-positive results and partnership concordance. Within the 83 partnerships, only one partner of nine (11%) index participants without evidence of C trachomatis infection at follow-up tested positive. In contrast, 52 partners of 74 (70%) index participants with evidence of C trachomatis infection at follow-up tested positive (prevalence ratio 6.3; 95% CI 0.98 to 40.8).
DISCUSSION
NAAT provides enhanced sensitivity to detect chlamydial infection. Understanding the clinical and public health implications of the additional infections identified by NAAT is critical for the appropriate use of these tests. Using concordance as an estimate of transmission, we observed that individuals who were positive by NAAT, but not by traditional assay, were significantly less likely than individuals who were positive by both NAAT and traditional assay to have a concordantly infected sexual partner. Nonetheless, partner concordance among individuals with infections detected only by NAAT was moderate (45%). In addition, a substantial proportion of individuals (17–22%) who screened positive by NAAT for C trachomatis in the emergency department setting had no evidence of chlamydial infection after a short follow-up period (median three weeks).
Key messages
Although the enhanced sensitivity of NAAT is well recognised, the significance and transmissibility of the additional infections detected by NAAT are unknown.
A substantial proportion of positive NAAT results for chlamydial infection may be of lower transmissibility and may not persist after a short follow-up.
Guidelines for testing, patient counselling and management should be formulated so that doctors, patients, and researchers are aware of the advantages of NAAT as well as its limitations.
A likely explanation for the diminished partner concordance among infections detectable only by NAAT is reduced organism burden. The enhanced sensitivity of NAAT increases the likelihood of detecting infections with relatively few organisms. Alternatively, NAAT may detect the “passive presence” of the organism after exposure, without a true, established infection. Consequently, individuals with infections detectable only by NAAT may be inherently less likely to transmit C trachomatis to their partners.
We observed a surprisingly high incidence of infection clearance, especially among women.10 This observation, coupled with our findings regarding reduced concordance among partners of index participants whose follow-up NAAT was negative, suggests that at least some NAAT infections may be cleared relatively rapidly, perhaps through antibiotic exposure or natural immune response,11 12 and not transmitted. We observed that many individuals without detectable infection at follow-up had been treated with antibiotics in the three months preceding their initial screening, suggesting that NAAT may have detected residual DNA, rather than viable organisms, at the initial screening evaluation.13 A proportion of the results could be false positives, although we re-tested all initial positive results to reduce this possibility. Sampling variability associated with the repeated testing of low-level infections is another possibility, but appears less likely because of the multiple specimens taken at follow-up.14 The likelihood of each of these possibilities is worthy of further clinical investigation.
The widespread application of NAAT has “resulted in considerable revision of our views of the clinical epidemiology of C trachomatis”.15 16 Only recently, however, have we begun to question the significance of some additional infections identified by NAAT.17 In this study, we examined partner concordance as a marker of the clinical significance of NAAT-identified infections. Further study of the association between asymptomatic NAAT-identified chlamydial infections and other clinical consequences, eg the incidence of pelvic inflammatory disease, or inflammation, is needed.
Few studies have examined infection transmission within partnerships.18 We chose a non-sexually transmitted infection clinic population as we were interested in understanding the transmissibility of largely asymptomatic, unrecognised C trachomatis infections. Consequently, we screened over 6000 individuals. In this cross-sectional sample, the timing of the prevalent infection in the index and the direction of transmission between index and partner could not be established. Generalisation of our findings may be constrained by our sample selection and by incomplete recruitment, although index participants had a similar risk profile to individuals who did not participate.
The advent of NAAT screening has expanded opportunities for prevention of the serious consequences of untreated C trachomatis infection. Although we strongly believe that individuals with a positive NAAT should be informed and treated, our study demonstrates that some NAAT-detected infections may not represent clinically active disease or transmissible infections. Failure to diagnose a chlamydial infection can negatively affect health, although incorrectly identifying individuals as infected can damage relationships. Patients, especially those with low-risk profiles or those screened from low C trachomatis prevalence populations,16 should be counselled about their test result accordingly. Guidelines for testing, patient counselling and management should be formulated so that users of this remarkable and powerful tool—doctors, patients, and researchers—are aware of the advantages of NAAT and also its limitations.
Acknowledgments
The authors would like to thank Don Orr, Martina Morris, and Heather Miller for serving as scientific advisors to this project. They also thank Sarah Mobius for her managerial contribution to the study and Sheping Li at RTI for programming and data management; Ambreen Khalil and Chadd Krauss for their oversight of interviews at the Johns Hopkins Adult Emergency Department; Joan Bess, Kenya S. Stewart and Nancy Willard of the Johns Hopkins Adolescent Health Research Group for outreach support; and Mary Ann Knott-Grasso, MS, CPNP, for providing patient care at the Johns Hopkins General Clinical Research Center. The authors also wish to thank the laboratory personnel from the Department of Medicine, University of North Carolina at Chapel Hill, including Marcia Stedman, John Schmitz, and Dana Lapple; and Jeff Younger, Billie Jo Wood, and Hope L Johnson from the Johns Hopkins School of Medicine, Department of Infectious Diseases.
REFERENCES
Footnotes
Funding: Primary support for this research was provided by National Institutes of Health (NIH) grant R01-HD039633 to SMR. RR was supported in part by a grant from NCRR NIH 3M01RR00052-39-5(S1).
Competing interests: None.
Author contributions: SMR, WCM, CFT, PL, JE, RR and DK contributed to the conception and design of the study. SMR, WCM, CFT, JE, JZ, RR, CG and MH contributed to the acquisition of data. SMR, WCM, MAV, AA-T and DK contributed to questionnaire design. SMR, MAV and LG contributed to data management. SR, WCM, MAV and CFT contributed to the analysis and interpretation of data. All authors contributed to writing the manuscript.
Role of the funding source: The National Institutes of Health did not participate in the design and conduct of the study, in the collection, analysis, and interpretation of the data, or in the preparation, review, or approval of the manuscript. The corresponding author had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Linked Articles
- Brief encounters