Article Text

Abstract
Objective: There has been much debate about the value of condoms in HIV/STI programming. This should be informed by evidence about intervention impact on condom use, but there is limited compiled literature. This review aims to quantify intervention impact on condom use in sub-Saharan Africa and Asia, in different types of partnership.
Methods: A systematic review was conducted of papers published between 1998 and 2006 presenting evaluations of interventions involving condom promotion in sub-Saharan Africa and Asia. Data on reported postintervention levels of condom use, and various measures of changes in condom use, by partnership type, were compiled.
Results: A total of 1374 abstracts were identified. Sixty-two met the inclusion criteria (42 reporting significant increases in condom use): 44 from sub-Saharan Africa and 18 from Asia. Many (19) reported on condom use in commercial sex (15 significant), six on use with casual partners (three significant), 11 on use in marital/steady partnerships (nine significant), 14 on use by youths (eight significant) and 20 combined partnership types (11 significant). There is substantial evidence of interventions targeted at sex workers and clients achieving large increases in condom use. Far less evidence exists of intervention impact on condom use in casual relationships. In primary partnerships, postintervention condom use was low unless one partner was knowingly HIV-infected or at high-risk, or avoiding pregnancy. Evaluations of interventions targeting youths recorded limited increases in condom use.
Conclusions: The findings illustrate the range of evidence about postintervention condom use in different partnerships, and how patterns of use are influenced by partnership type and perceptions of risk. Where possible, intervention studies should also assess biological endpoints, since prevention of infection is the measure of most interest in the evaluation of condom promotion interventions.
- RCT, randomised controlled trial
Statistics from Altmetric.com
Condoms are an effective method of HIV prevention, as illustrated by evidence from sero-discordant couple studies.1,2 However, recently the relative importance of condom promotion in comparison with promoting abstinence or partner reduction has been debated.3–5
The overall impact of condoms will be a combination of their biological protection and level of use in different partnerships. The former has been explored in detail, with two reviews concluding that consistent and inconsistent condom use reduces the annual HIV incidence in sero-discordant couples by 85%1 and 69%,2 respectively. There is far less compiled evidence on the degree to which interventions can increase condom use in different populations. Most global evidence on condom use comes from population or targeted behavioural surveys.6–10 However, as it is often unclear whether respondents have had recent intervention contact, the findings represent an average across exposed and unexposed individuals.
Key messages
-
It is possible to significantly increase condom use in commercial, casual, marital/steady and youth sexual partnerships
-
The magnitude of the increase in condom use, and the level of use achieved, are strongly influenced by partnership type and perceptions of risk, with findings often being remarkably consistent across African and Asian settings
-
Where possible, biological endpoints should also be assessed in the evaluation of condom promotion interventions, to limit the biases inherent in self-reports of condom use, and since prevention of infection is the measure of most interest
-
This review supports the continued promotion of condoms as part of a comprehensive response to the global HIV epidemic
To date there has been no systematic review of postintervention levels of condom use across different geographical settings and partnership types. Hearst and Chen reviewed literature on condom efficacy and use in developing countries, but mostly described selected case studies.11 Other reviews have tended to summarise the impact of different HIV prevention interventions in the US12–16 or developing countries,17–20 among adolescents,21 long-distance truck drivers,22 or people living with HIV.23,24 This paper presents a systematic review of published evidence on the impact of intervention contact on the levels of condom use in different partnerships in sub-Saharan Africa and Asia.
METHODS
The systematic review aimed to identify published journal articles of HIV/STI/pregnancy prevention interventions implemented in sub-Saharan Africa or Asia. For logistical reasons, only papers written in English were reviewed. Six databases were searched: PubMed, MEDLINE, Cochrane Library, BIDS CAB Abstracts, EMBASE and POPLINE. The database search was undertaken dynamically, adding in more MeSH (Medical Subject Headings) or “free-text” search terms iteratively and narrowing the number of databases searched to those identifying the most articles of interest for the review (appendix 1). Randomised controlled trials (RCTs) provide the strongest form of evidence about intervention impact. However, due to the small number of RCTs identified in preliminary searches, this review also includes studies with less rigorous designs, including pre–post intervention comparisons, and postintervention comparisons with “control” populations. All searches were conducted within the publication date limits of January 1998–September 2006, reflecting the aim to capture relatively recent evidence and to reduce the scope of work.
In total, 1374 distinct articles were identified. Abstracts were scanned to decide if they met the inclusion criteria (appendix 2), and the findings on reported male condom use during penile–vaginal sexual intercourse in different partnership types were then summarised.
If several condom measures were available, the most useful for the review was recorded. For example, “ever use” was only recorded if no other data were available, and use at “last sex act” was recorded in preference to “consistent use”, since the latter may be subject to recall bias and is less comparable across studies due to the use of different reference periods. Where distributions provided the only available condom use data, the “always” category was recorded. The increases in condom use presented were drawn directly from the published papers, and so were affected by the study design and statistical methods used. In some studies, this was restricted by the statistical comparisons presented in the articles. For articles where no statistical tests were used, the significance of any change in condom use was tested through a comparison of two proportions. Where several significant increases in condom use were reported in the article, the largest increase is presented.
RESULTS
A total of 1374 distinct abstracts were identified. Sixty-two met the inclusion criteria: 44 from sub-Saharan Africa25–68 and 18 from Asia.69–86 Many (19) reported on condom use in commercial sex,26,28,33–35,39,50,51,58,69,71,73,75–77,80,84–86 six on use with casual partners,25,41,60,65,79,86 11 on use in marital/steady partnerships,34–37,49,51,68,78,79,83,86 14 on use by youths27,29,43–45,47,48,52,54,55,57,59,64,74 and 20 combined partnership types.30–32,38,40,42,46,53,56,60–63,65–67,70,72,81,82 Twelve studies investigated condom use in more than one partnership type.26,34–36,39,41,51,60,65,71,79,86
Condom use did not increase significantly (p>0.05) in 16 of the studies reviewed.52,53,55–57,59–68,86 Additionally, four papers reported significant increases in condom use but concluded that these were not attributable to the intervention.54,58,84,85 Of these 20 studies, six targeted youths,52,54,55,57,59,64 10 were community-based,53,56,58,60–62,65,67,68,86 two targeted sex workers84,85 and two targeted women using postabortion or safe motherhood services63,66. Factors cited as diminishing the likelihood of documenting a significant increase include small sample sizes,53,57,65,86 the use of very short or long follow-up periods,52,76 no adequate control group,60,61 high preintervention levels of condom use,54,84,85 or contextual changes that undermined the intervention.84,85
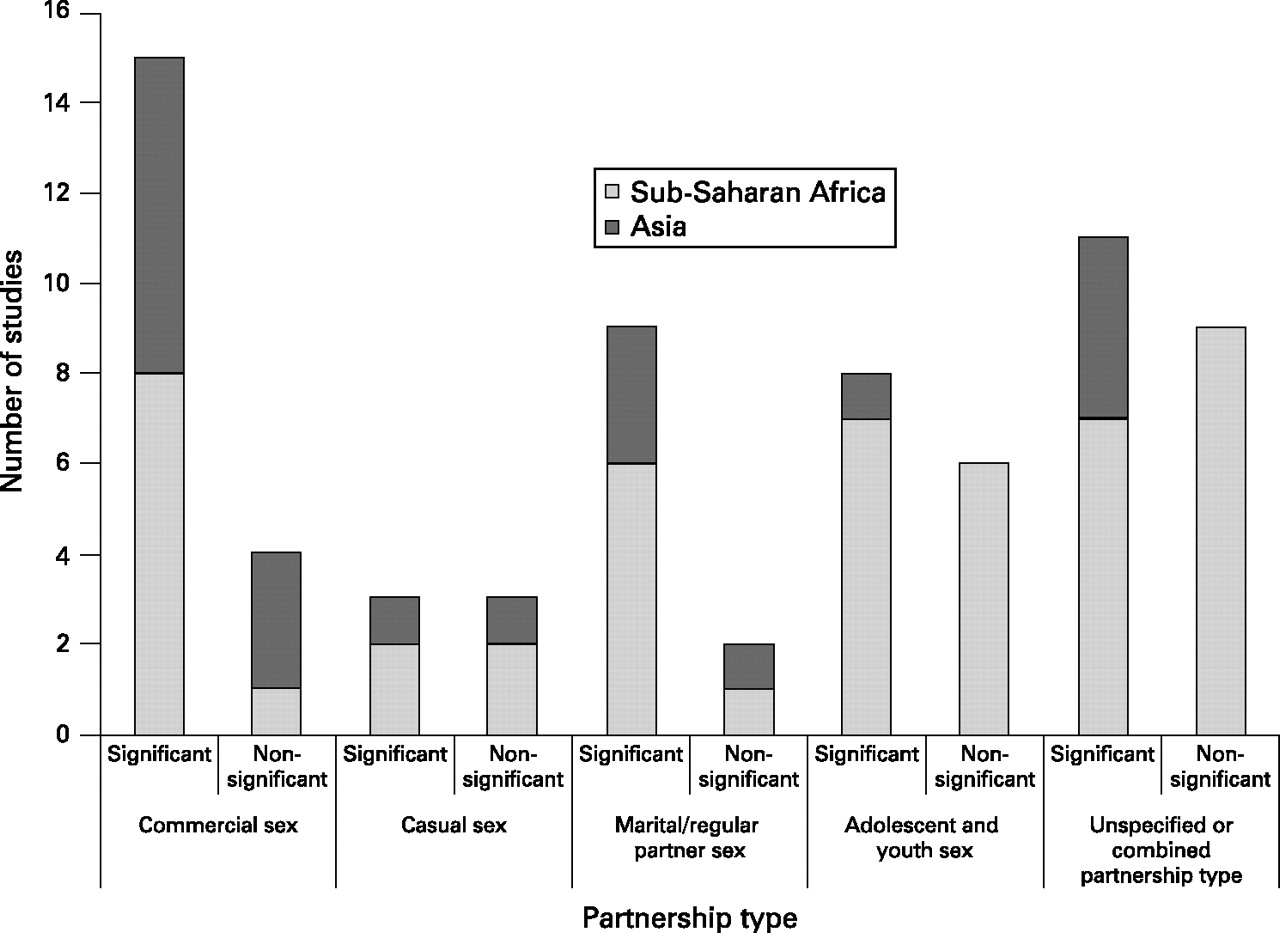
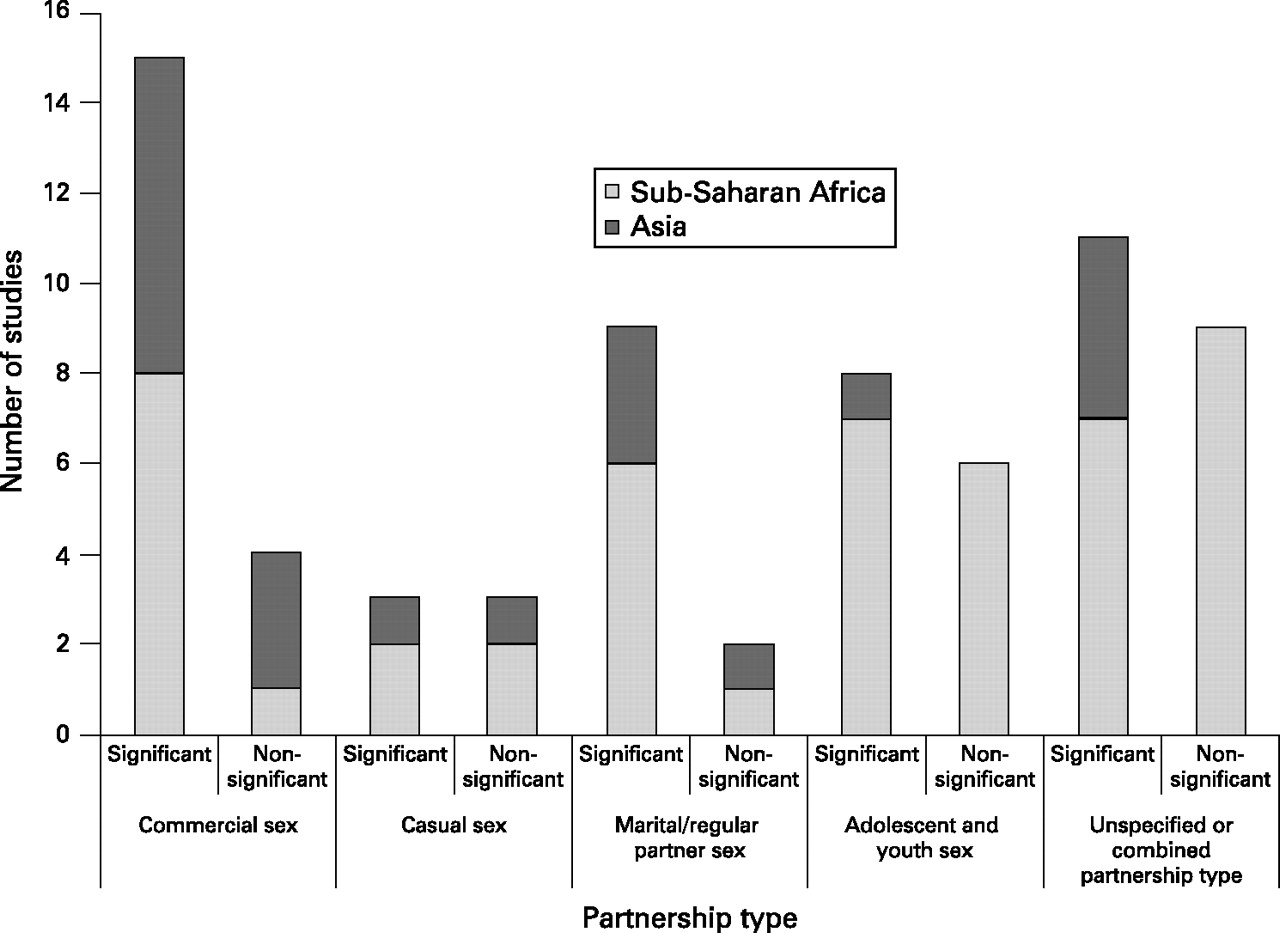
While more studies reporting significant increases in condom use measured use during commercial sex than in any other type of partnership, most papers reporting no significant change in condom use were evaluating interventions targeting youths or the general population (fig 1). Interventions seemed particularly effective at increasing condom use when they involved peer or other health education, and targeted high-risk populations such as sex workers and their clients (table 1).
Summary of studies with significant and non-significant differences in condom use by partnership type, target group and intervention type
{kind=link}
Comparison of studies with significant and non-significant differences in condom use by region and partnership type.
Commercial sex
Fifteen of the 19 studies of condom use in commercial sex reported significantly increased levels of condom use (table 2). In eight of these, reported condom use more than doubled,28,33–35,69,71,76,80 and in seven, high postintervention levels of reported condom use were documented (>70% use by measure utilised).28,51,69,73,76,77,80 All these highly successful interventions involved some combination of peer or other health education, condom provision and/or STI testing and treatment. However, all the results are from pre-post intervention comparison, with no control-group comparison. Relatively low postintervention levels of condom use (19–56% use in last sex or last five acts, 41–58% consistent use) were recorded in five studies, but the increase in condom use was significant.33–35,71,75 Three of these targeted high-risk men,35,71,75 another targeted women and truckers in Tanzania,34 and the fifth offered risk-reduction counselling, STI treatment and condoms to sex workers in Kenya.33 Again, only pre–post comparisons are presented, except in one non-randomised controlled trial (NRCT) among high-risk men in the Philippines.75
Casual sex
Six studies reported intervention impact on condom use with casual or non-regular sexual partners, with three documenting significant increases (table 2). One of these compared condom use at last sex by level of intervention exposure,25 and two measured “always” condom use in a pre–post intervention comparison.41,79 All three studies reported that condom use increased to a moderate level (25–48% use by measure utilised).
Marital/steady and regular partner sex
Of the 11 studies reporting data on condom use with marital/steady or regular partners, nine reported a significant increase in condom use (table 2). However, only two of the significant studies were among low-risk populations—married women in Thailand.78,83 One reported very low levels of consistent condom use (5% at the 6-month follow-up) following counselling, HIV testing and condom use,83 whereas in the other, 58% of individuals reported using condoms “more frequently” with their spouse.78 Although this latter study was a cluster-RCT, the measure of condom use was weak.
Among primary partnerships with an acknowledged higher risk of HIV, interventions did increase condom use substantially,34–37,49,51,79 but often only to fairly low postintervention levels (24–33% use in last sex or consistent use).36,49,51 The exceptions included an intervention among HIV-discordant couple-cohorts in Rwanda,37 and peer education and condom promotion among male transport workers in Senegal and Tanzania who frequently had multiple partners.34,35 In addition, high levels of condom use in regular partnerships were reported postintervention among three ethnic groups in a Chinese study,79 who were potentially using condoms for contraception.
Adolescent and youth sex
Fourteen studies measured intervention impact on condom use by youth (only one of which was from Asia). Eight of these documented small yet significant increases in reported condom use (table 2) (6–19% absolute increase).27,29,43–45,47,48,74 Five reported significant increases in reported condom use at last sex, with the reported postintervention condom use at last sex ranging from 31 to 78%.27,43–45,48 The greatest postintervention condom use (78% use in last sex) was reported in an individual-RCT among secondary school students in Namibia who had received HIV/AIDS education, and training in communication and decision-making skills.27 Otherwise, a cluster-RCT observed a significant difference in “some” condom use at follow-up (39% vs 32%),47 and two other studies reported high levels of “ever use” (97% and 55% postintervention).29,74
Partner type is aggregated or unspecified
Twenty intervention studies combined partnership types or did not specify the type of partnership in which condoms were used. Eleven of these reported significant increases in condom use (table 2). Five reported condom use at last sex,40,42,46,72,81 with three finding levels of use of 42% or lower,40,72,81 and the rest involved Voluntary Counselling and Testing (VCT) with reported high levels of use (71–85%) postintervention.42,46 Only one study measured “always” use of condoms, and reported an increase from 3% to 8% following a multifaceted intervention for young adults in a semirural township in China (comparing control versus intervention townships postintervention).82 However, there was no significant difference in reported condom use at last sex between the intervention and control groups (p>0.05).82
Impact across partnership type
Twelve studies assessed intervention impact on condom use in more than one type of partnership,26,34–36,39,41,51,60,65,71,79,86 nine of which found significant increases in at least one partnership type.26,34–36,39,41,51,71,79 Three of these reported a significant increase for use in commercial sex following intervention activities, but not with non-commercial partners.26,39,71 Four reported significant increases for both commercial/casual and regular partnerships.34,35,51,79 One study, in which the sample size of sex workers was small, found a significant increase in condom use in casual partnerships but not in commercial sex.41 Another found a significant increase in condom use between men and their wives but not with their other partners with whom condom use was already high.36
Evidence of other forms of impact
There has been concern that condom promotion may increase sexual risk-taking, especially among youth, adversely affecting the overall impact of condom promotion campaigns.87,88 Of the 19 studies that provided data on the number of sexual partners, a significant decline was reported postintervention in 13,31,33,35,36,38,41,43,44,71,76,77,79,81 with four others finding no significant difference in the number of sexual partners reported,27,29,39,82 and only one observing an increase in the number of clients per day.28 From the studies that focused on youth, five found no evidence that non-sexually active youths became active as a consequence of the intervention,27,29,43,44,74 and only one reported a significant increase in the proportion of male youth who were sexually active following a 2-year intervention.48 Although not generally reported, it is possible that other risk behaviours may increase, such as selecting higher-risk partners, and so this too should be monitored in evaluation studies.
DISCUSSION
Well-designed intervention studies can provide invaluable evidence about how different interventions may impact on condom use in different settings, and in different forms of sexual partnership. It was hoped that, by focusing on peer-reviewed publications, the quality of studies reviewed would be assured, although in practice, the quality of the evidence varied widely. Only six of the 42 studies presented in table 2 were RCTs,27,29,40,47,51,78 and two others randomised communities to intervention or control conditions69,82. Unfortunately, four of the RCTs29,40,51,69 and four of the NRCTs31,32,73,79 presented only pre–post comparisons rather than significance testing of the male condom intervention group versus the control group at follow-up. Otherwise, most studies did not include a control group, or did not randomly allocate to intervention and control groups, which may limit the reliability of conclusions about intervention effect. For the studies with no comparison group, some of the observed increases in condom use may also reflect underlying temporal effects, in addition to intervention effects.9,10 The focus on published reports may have also led to a publication bias towards studies showing impact.
Fundamentally, the conclusions from the review will be limited by the degree to which condom use is accurately reported. There may be inaccuracies from reporting bias due to social desirability compelling participants to over-report condom use, since they are part of a project in which condoms are promoted, or to under-report condom use if condoms are stigmatised in the population.89 Some studies attempted to validate self-reported sexual behaviour data through the inclusion of biological endpoints.26,28,33,40,41,69,71,76,77,80 The majority of these reported significant declines in the prevalence/incidence of HIV26,28,71 or other STIs,26,28,33,71,76,80 while one found only minor differences in STI prevalence between consistent and inconsistent users,40 and another had baseline rates of STIs that were too low to demonstrate any change.69 Significant increases in HIV/STI prevalence were reported in two of the studies,41,77 with the authors of one suggesting that a history of condom use was likely to be a marker for more frequent commercial sex,77 and the other concluding that the findings emphasise the need for a broad range of interventions alongside political and social engagement.41 When considering this evidence, it is important to keep in mind that condom effectiveness against an STI depends on the infectivity of that specific STI.90 Other methods of validation included asking both male and female partners about their condom use,37,80 or comparing the reported coital frequency and condom use data with the number of condoms distributed.40
Although UNAIDS and other agencies have invested in methodological research to identify how best to enquire about condom use,89 several imprecise measures were used in the studies reviewed. It may be that increased use at last sex reflects greater uptake of condoms by non-users, while increased consistency of use may reflect increased use by existing users. The lack of standardised measures of condom use meant that summary measures of impact could not be developed. As over a quarter of the studies examined combined partnership types, there were also limitations about the degree to which intervention impact on condom use in different forms of relationship could be assessed. Those studies that did specify the partnership type were grouped accordingly, despite the heterogeneity of the studies in each group, which varied by target population, intervention type, geographic area and baseline levels of condom use. Had more studies met the inclusion criteria, these could have perhaps formed more homogenous sub-groups for comparison within each partnership type.
Despite these limitations, this review provides an overview of current evidence. There is substantial evidence of interventions targeted at sex workers and their clients, in both African and Asian contexts, achieving significant large increases in condom use. These interventions seem to primarily utilise peer or other health education combined with STI testing and treatment. Further research is needed to disentangle the factors influential on the largest gains in condom usage.
There is far less evidence about intervention impact on levels of condom use in casual sexual relationships. This lack of evidence makes it impossible to draw any conclusions and highlights the need for further evaluation studies in this area, particularly since, in many parts of the world, casual sex is a potentially important mechanism for HIV transmission.
In primary partnerships, postintervention condom use was generally low unless one partner was knowingly HIV-infected or at high risk, or avoiding pregnancy. The evidence suggests that increased condom use among primary partnerships is most feasible if the perception of risk of an unwanted outcome (ie, HIV/STI infection or pregnancy) is high, although the stigma of HIV may also influence behaviour. More studies of condom use in long-term partnerships following interventions targeted at low-risk groups are required.
There was mixed evidence of the impact of condom promotion among youth. Compared with other target populations, interventions among youths recorded a lower increase in condom use. However, high levels of use are possible. Geographically the evidence is skewed, as only one study focused on Asia. The lack of data highlights the need for further evaluations of interventions for youths, particularly in Asia. Such interventions should draw upon a recent review conducted by WHO, identifying the forms of intervention for adolescents that are most promising.21 Promoting condoms for contraception may increase use among young people, as Cleland and Ali (2006) found that, across 13 African countries, pregnancy prevention can be an important motivating force for condom use by young single women.9
Gender differences were also noted. In five of the articles included in the review, condom use increased significantly among males but not females within the same study,30,31,43,44,49 while only one study found the reverse among youths.47 This highlights that condom use depends on male cooperation.
CONCLUSION
To date, the debate about condom promotion and use has been largely fuelled by political rhetoric, with insufficient attention paid to the impact of interventions on the magnitude of the change in condom use in different sexual partnerships and settings. This review highlights that it is possible to significantly increase condom use in commercial, casual, marital/steady and youth sexual partnerships. However, it also illustrates that the magnitude of the increase in condom use, and the level of use achieved, are strongly influenced by partnership type and perceptions of risk, with findings often being remarkably consistent across African and Asian settings.
There is clearly a need for further evaluation studies of condom promotion interventions, particularly of their impact on use in casual sex, in marital sex among low-risk groups, and of those targeting youths in Asia. Where possible, biological endpoints should also be assessed to limit the biases inherent in self-reports of condom use, and since prevention of infection is the measure of most interest in the evaluation of condom promotion interventions. The synthesis of data across studies would be facilitated if standardised condom use measures were used. As HIV risk often differs by partnership type, and different programmatic focuses may be needed to increase condom use in different forms of sexual partnership, it is important that evaluations collect data on condom use in different types of relationships, to enable lessons to be learned for future HIV/STI programming. Evaluations should both report on condom use at last sex with each partner and estimate the extent to which consistent condom use is being achieved in each type of partnership over a specified reference period, since achieving consistent condom use may be particularly important in terms of HIV/STI prevention.91,92
This review illustrates that it is possible to increase condom use significantly in different types of sexual partnership, and across different continents, and so supports the continued promotion of condoms as part of a comprehensive response to the global HIV epidemic.
Acknowledgments
This work was funded by the Global Campaign for Microbicides at the Program for Appropriate Technology in Health (PATH), International Family Health via a grant from the European Community, the DFID Knowledge Programme on HIV/AIDS & STI, and the DFID Research Programme Consortium for Research and Capacity Building in Sexual & Reproductive Health & HIV in Developing Countries. The views and opinions expressed are those of the authors alone and can therefore in no way be taken to reflect the official opinion of the London School of Hygiene and Tropical Medicine, DFID, PATH, the European Commission or International Family Health. We would like to thank John Eyers and Debbie Pledge for their information specialist expertise and advice, Lori Heise for her helpful input, and the useful feedback received from several peer-reviewers.
CONTRIBUTIONS
AF took the lead in the review process and made substantial contributions to the conception, design, analysis and interpretation of the results presented. AF conducted the searches for articles published 1998–2003 and identified studies that met the inclusion criteria. AF produced the first draft of the review paper. MH conducted the searches for articles published 2003–2006 and identified studies that met the inclusion criteria. MH revised the draft paper with the additional articles she had identified, developed the summary figure (fig 1) and table (table 1), and contributed to the interpretation of the results. PV and CW contributed to the development of the search strategy and inclusion criteria, and helped to interpret the findings. PV and CW provided substantial input into several drafts of the paper.
REFERENCES
Supplementary materials
web only appendix 83/7/510
Files in this Data Supplement:
web only table 83/7/510
Files in this Data Supplement:
Footnotes
-
Competing interests: None declared.
Linked Articles
- Brief Encounters