Article Text

Statistics from Altmetric.com
We thought Journal readers might be interested to hear about a patient we saw recently in our clinic. A 35-year-old woman attended for a routine change of Mirena® intrauterine system (IUS). Since the insertion of the IUS 5 years before, she had colposcopy for an abnormal (CIN 2) smear and the cervical lesion was cauterised. On insertion of the speculum, the threads were clearly visible but on attempting removal, the opening of the os was noted to be stenosed. The threads of the IUS were caught using sponge forceps and moderate traction was required to remove the device. It was quite a difficult removal although not overtly so. However, on removal of the IUS, its appearance was unusual (Figure 1A). It appeared to have been removed without the outer hormone sleeve that would usually sit around the IUS stem. The IUS was not replaced and the patient was referred to the gynaecological outpatient clinic.

{kind=link}
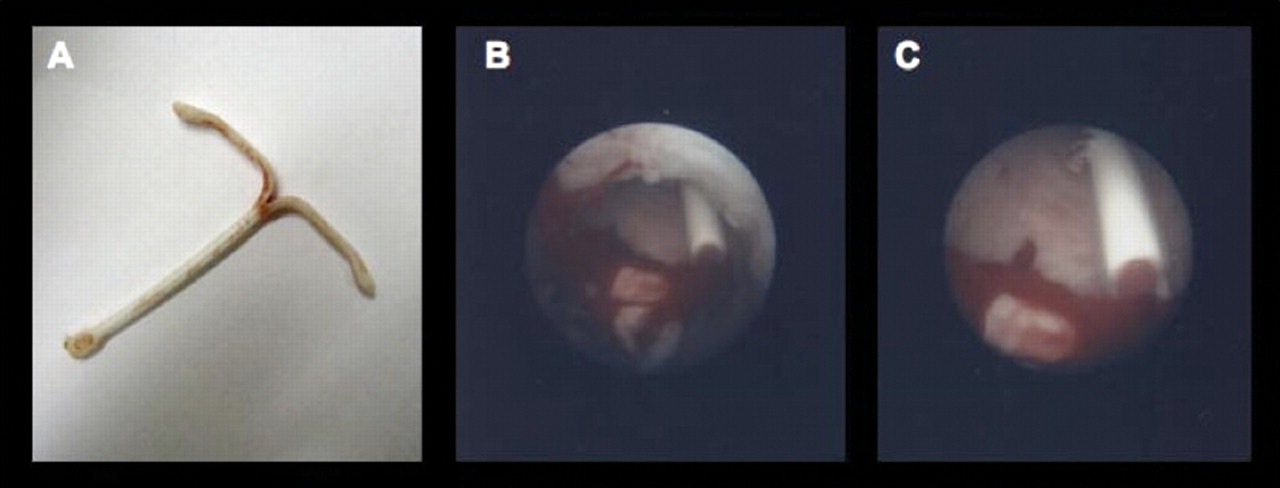
(A) Mirena® intrauterine system without hormone sleeve, (B) hormone sleeve in uterine cavity and (C) hormone sleeve in uterine cavity.
At this clinic, a pelvic ultrasound scan confirmed the presence of the outer hormone sleeve of the IUS in the uterine cavity. Due to the marked stenosis of the cervix, it was not possible to attempt removal of the sleeve and arrangements were made for hysteroscopy and removal of outer sleeve under anaesthetic.
In theatre, the cervix was noted to be markedly stenosed and required dilatation using Hegar's dilators. Once the cervix was dilated, hysteroscopy was performed. At hysteroscopy, the retained outer sleeve was easily located lying loose in the endometrial cavity (Figure 1B, 1C). This was grasped with toothed forceps via the hysteroscope and removed. It was examined and found to be intact with no evidence of any split in the sleeve. At the patient's request, a new IUS was inserted.
A complication of cautery to the cervix is cervical stenosis and this is said to be present if the cervical canal diameter is less than 2.5 mm.1 In this case, the patient had colposcopy for an abnormal smear 2 years after the insertion of the IUS and required treatment with cervical cautery causing a very tight cervical stenosis.
Removal of an IUS is normally very straightforward. Following insertion of a Cusco's speculum, the threads of the IUS can be seen protruding through the cervical os. These threads are caught with a pair of sponge-holding forceps and gentle traction will extract the device.
In this case, because of the cervical stenosis, as the device was being removed the outer hormone sleeve slipped over the IUS arms and became free, remaining in the uterine cavity. Extra care should be taken when removing an IUS if the cervix has been cauterised since insertion.
Following removal of the IUS, it is essential that the device be inspected to ensure that it has been removed completely. In most cases, the device will be removed easily and appear normal. Very occasionally the outer hormone sleeve will slip up over the horizontal arms during removal but the knobs at the end of these arms will usually prevent the outer sleeve slipping off completely. In such a situation the IUS can still be removed complete. Should the outer hormone sleeve slip over the arms and remain in the uterine cavity, as occurred in this case, the patient should be referred to the gynaecological outpatient clinic for further management.
Patient satisfaction with the Mirena IUS is very high with 95% or more users greatly satisfied.2 Despite the difficult removal due to the presence of cervical stenosis, this patient was sufficiently satisfied to request insertion of a new IUS once the displaced outer hormone sleeve had been removed. In conclusion, this case highlights the importance of checking that the IUS is intact and complete following removal.
Footnotes
-
Competing interests None.